UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM 10-K
ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the Fiscal Year Ended December 31, 2013
Commission File Number 001-36019
TONIX PHARMACEUTICALS HOLDING CORP.
(Exact name of registrant as specified in its charter)
|
Nevada
|
|
26-1434750
|
|
(State or other jurisdiction of incorporation
or organization)
|
|
(IRS Employer Identification No.)
|
|
|
|
|
|
509 Madison Avenue, Suite 306
New York, New York
|
10022
|
(212) 980-9155
|
|
(Address of principal executive office)
|
(Zip Code)
|
(Registrant’s telephone number, Including area code)
|
Securities registered pursuant to Section 12(b) of the Act:
|
Title of each class
|
Name of each exchange on which registered
|
|
Common Stock, $0.001 par value
|
The NASDAQ Capital Market
|
Securities registered pursuant to Section 12(g) of the Act: None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined by Rule 405 of the Securities Act. Yes ¨ No x
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or 15(d) of the Act. Yes ¨ No x
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes x No ¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§ 229.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes x No ¨
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K (§229.405 of this chapter) is not contained herein, and will not be contained, to the best of the registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. ¨
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See definitions of “large accelerated filer,” “accelerated filer” and “smaller reporting company” in Rule 12b-2 of the Exchange Act.
|
Large accelerated filer ¨
|
Accelerated filer ¨
|
|
Non-accelerated filer ¨
|
Smaller reporting company x
|
|
(Do not check if a smaller reporting company)
|
|
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act).Yes ¨ No x
The aggregate market value of the voting common equity held by non-affiliates as of June 28, 2013, based on the closing sales price of the Common Stock as quoted on The Nasdaq Capital Market was $9,146,524. For purposes of this computation, all officers, directors, and 5 percent beneficial owners of the registrant are deemed to be affiliates. Such determination should not be deemed an admission that such directors, officers, or 5 percent beneficial owners are, in fact, affiliates of the registrant.
As of March 24, 2014, there were 9,899,497 shares of registrant’s common stock outstanding.
TABLE OF CONTENTS
|
|
|
|
|
PAGE
|
|
|
PART I
|
|
|
|
|
|
|
|
Item 1.
|
|
Business
|
|
3
|
|
|
Item 1A.
|
|
Risk Factors
|
|
25
|
|
|
Item 1B.
|
|
Unresolved Staff Comments
|
|
42
|
|
|
Item 2.
|
|
Properties
|
|
42
|
|
|
Item 3.
|
|
Legal Proceedings
|
|
42
|
|
|
Item 4.
|
|
Mine Safety Disclosures
|
|
42
|
|
|
|
|
|
|
|
|
|
PART II
|
|
|
|
|
|
|
|
Item 5.
|
|
Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities
|
|
43
|
|
|
Item 6.
|
|
Selected Financial Data
|
|
43
|
|
|
Item 7.
|
|
Management’s Discussion and Analysis of Financial Condition and Results of Operations
|
|
44
|
|
|
Item 7A.
|
|
Quantitative and Qualitative Disclosures about Market Risk
|
|
49
|
|
|
Item 8.
|
|
Financial Statements and Supplementary Data
|
|
F-1 – F-24
|
|
|
Item 9.
|
|
Changes in and Disagreements with Accountants on Accounting and Financial Disclosures
|
|
50
|
|
|
Item 9A.
|
|
Controls and Procedures
|
|
50
|
|
|
Item 9B.
|
|
Other Information
|
|
50
|
|
|
|
|
|
|
|
|
|
PART III
|
|
|
|
|
|
|
|
Item 10.
|
|
Directors, Executive Officers and Corporate Governance
|
|
51
|
|
|
Item 11.
|
|
Executive Compensation
|
|
55
|
|
|
Item 12.
|
|
Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters
|
|
58
|
|
|
Item 13.
|
|
Certain Relationships and Related Transactions, and Director Independence
|
|
59
|
|
|
Item 14.
|
|
Principal Accounting Fees and Services
|
|
60
|
|
|
|
|
|
|
|
|
|
PART IV
|
|
|
|
|
|
|
|
Item 15.
|
|
Exhibits, Financial Statement Schedules
|
|
61
|
|
|
|
|
|
|
|
|
|
|
|
Signatures
|
|
63
|
|
PART I
ITEM 1 - BUSINESS
This Annual Report on Form 10-K (including the section regarding Management's Discussion and Analysis of Financial Condition and Results of Operations) contains forward-looking statements regarding our business, financial condition, results of operations and prospects. Words such as “expects,” “anticipates,” “intends,” “plans,” “believes,” “seeks,” “estimates” and similar expressions or variations of such words are intended to identify forward-looking statements, but are not deemed to represent an all-inclusive means of identifying forward-looking statements as denoted in this Annual Report on Form 10-K. Additionally, statements concerning future matters are forward-looking statements.
Although forward-looking statements in this Annual Report on Form 10-K reflect the good faith judgment of our Management, such statements can only be based on facts and factors currently known by us. Consequently, forward-looking statements are inherently subject to risks and uncertainties and actual results and outcomes may differ materially from the results and outcomes discussed in or anticipated by the forward-looking statements. Factors that could cause or contribute to such differences in results and outcomes include, without limitation, those specifically addressed under the heading “Risks Factors” below, as well as those discussed elsewhere in this Annual Report on Form 10-K. Readers are urged not to place undue reliance on these forward-looking statements, which speak only as of the date of this Annual Report on Form 10-K. We file reports with the Securities and Exchange Commission (“SEC”). You can read and copy any materials we file with the SEC at the SEC's Public Reference Room at 100 F Street, NE, Washington, DC 20549. You can obtain additional information about the operation of the Public Reference Room by calling the SEC at 1-800-SEC-0330. In addition, the SEC maintains an Internet site (www.sec.gov) that contains reports, proxy and information statements, and other information regarding issuers that file electronically with the SEC, including us.
We undertake no obligation to revise or update any forward-looking statements in order to reflect any event or circumstance that may arise after the date of this Annual Report on Form 10-K. Readers are urged to carefully review and consider the various disclosures made throughout the entirety of this annual Report, which attempt to advise interested parties of the risks and factors that may affect our business, financial condition, results of operations and prospects.
This Annual Report on Form 10-K includes the accounts of Tonix Pharmaceuticals Holding Corp. (“Tonix”) and its wholly-owned subsidiaries, as follows, collectively referred to as “we”, “us” or the “Company”: Tonix Pharmaceuticals, Inc., a Delaware corporation ("Tonix Sub"), Krele LLC, a Delaware limited liability company ("Krele"), Tonix Pharmaceuticals (Canada), Inc., a corporation incorporated under the laws of the province of New Brunswick, Canada ("Tonix Canada") and Tonix Pharmaceuticals (Barbados) Ltd., a corporation incorporated under the laws of Barbados ("Tonix Barbados"). Tonix Sub is a wholly-owned subsidiary of Tonix, and Krele, Tonix Canada and Tonix Barbados are wholly-owned subsidiaries of Tonix Sub.
Corporate Structure
We were incorporated on November 16, 2007 under the laws of the State of Nevada as Tamandare Explorations Inc. From inception through October 2011, we were involved in the acquisition, exploration and development of natural resource properties in the State of Nevada. On October 7, 2011, we executed and consummated the Share Exchange.
In the Share Exchange, the Tonix Shareholders exchanged their shares of Tonix Sub for newly issued shares of common stock. As a result, upon completion of the Share Exchange, Tonix Sub became our wholly-owned subsidiary.
Upon completion of the Share Exchange, the Tonix Shareholders received an aggregate of 1,133,334 shares of our common stock. 75,000 shares of common stock were returned to us from the prior officer, which were retired, and our existing shareholders retained 200,000 shares of common stock. The 1,133,334 shares issued to the Tonix Shareholders constituted approximately 85% of our 1,333,334 issued and outstanding shares of common stock immediately after the consummation of the Share Exchange.
As a result of the Share Exchange, we acquired 100% of the capital stock of Tonix Sub and consequently, control of the business and operations of Tonix Sub and Krele. From and after the consummation of the Share Exchange, our primary operations consist of the business and operations of Tonix Sub and Krele.
On October 11, 2011, we changed our name to Tonix Pharmaceuticals Holding Corp. to reflect our new business.
Corporate Background
In 1996, Seth Lederman, MD, and Donald Landry, MD, PhD, formed L & L Technologies LLC, or L&L, to develop medications for central nervous system, or CNS, conditions. Dr. Lederman is our Chairman and Chief Executive Officer and Dr. Landry is a Director. L&L was a founder of Janus Pharmaceuticals, Inc., which later became Vela Pharmaceuticals, Inc., or Vela, which developed various therapeutics, including a very low dose, or VLD, version of cyclobenzaprine, or CBP, under an agreement with L&L. Vela decided to focus its resources on other programs and transferred the rights to VLD CBP and certain other technologies to L&L in March 2006.
Tonix Sub formed in June 2007 as Krele Pharmaceuticals, Inc. by L&L and Plumbline. Dr. Lederman is Managing Partner of Plumbline. Plumbline possessed rights to certain technology for the treatment of alcohol dependence and abuse. In connection with founding Tonix Sub, L&L and Plumbline entered into an intellectual property transfer and assignment agreement with Tonix Sub for the purpose of assigning patents and transferring intellectual property and know-how in exchange for shares of common stock of Tonix Sub. As a result of economic conditions related to the financial crisis of 2007 and 2008, Tonix Sub was not successful in raising money to fund its programs until 2009. As a result, Tonix Sub was unable to advance the development programs and had little activity except for prosecuting and maintaining patents and maintaining contracts.
In 2009, Tonix Sub contracted with the Toronto Psychiatric Research Foundation to analyze the sleep data from a Phase 2a trial of nighttime VLD CBP in fibromyalgia, or FM (“the Moldofsky Study”). The Moldofsky Study was conducted in Canada by the Toronto Psychiatric Research Foundation, and Tonix Sub obtained the data from this study from L&L. In addition, in 2009, Tonix Sub contracted with Caliper Life Sciences Inc., or Caliper, to analyze the interactions of CBP with certain receptors. In June 2010, Tonix Sub entered into consulting agreements with L&L and Lederman & Co., LLC, or Lederman & Co, and also acquired certain rights to develop isometheptene mucate as a treatment for certain types of headaches from Lederman & Co, which we are developing as TNX-201. Dr. Lederman is managing partner of Lederman & Co. Between June 2010 and October 2011, Tonix Sub was active in recruiting new officers and directors and initiating preclinical and clinical development of novel CBP formulations.
In July 2010, Tonix Sub changed its name to Tonix Pharmaceuticals, Inc. In August 2010, we formed Krele to commercialize products that are generic versions of predicate New Drug Application, or NDA, products. We anticipate that when our branded products lose patent protection, Krele may market authorized generic versions of them. Krele also may develop or acquire generic products approved under ANDAs and we may market branded versions (branded generics) of such products. Krele has been issued a state license in New York.
On April 23, 2013, we formed Tonix Canada. Tonix Canada is intended to perform research and development efforts in Canada. As a Canadian entity, we expect Tonix Canada will be entitled to receive certain reimbursable tax credits for research expenditures in Canada.
On October 24, 2013, Tonix Sub formed Tonix Barbados. On December 31, 2013, Tonix Barbados entered into a license agreement and a cost-sharing agreement with Tonix Sub, pursuant to which Tonix Barbados acquired the rights to develop and commercialize TNX-102 SL and TNX-201 for non-US markets in exchange for (1) cost sharing of research and development costs going forward and (2) royalties of 8% and 6% on net sales of TNX-102 SL and TNX-201, respectively.
Business Overview
We are a pharmaceutical company dedicated to the development of novel pharmaceutical products for challenging problems. Our lead drug development programs are directed toward CNS conditions that manifest with pain that originates in the brain, or central pain. Central pain results from abnormal sensory processing in the CNS, rather than from dysfunction in peripheral tissues where pain is perceived. Our most advanced development program is for the management of fibromyalgia, or FM, a central pain syndrome. We also have development programs for the management of post-traumatic stress disorder, or PTSD, in which central pain is a component, and for the relief of episodic tension-type headache, or ETTH. We also have a pipeline of additional product candidates that we plan to develop for other CNS indications.
TNX-102 SL
Our lead product candidate, TNX-102 sublingual tablet, or TNX-102 SL, is a small, rapidly disintegrating tablet containing CBP for sublingual administration. We are developing TNX-102 SL as a bedtime therapy for the management of FM and PTSD. CBP is the active pharmaceutical ingredient of two widely prescribed products, and we are pursuing the development of TNX-102 SL for indications distinct from those for which current CBP products are approved. We believe that TNX-102 SL is an optimized CBP product for the treatment of FM and PTSD, and is distinct from current CBP products in three ways: (1) it is being developed at a dose level significantly below the lowest marketed doses of current CBP products; (2) it is placed under the tongue, to disintegrate, dissolve and provide sublingual absorption, whereas current CBP products are swallowed and provide absorption in the small intestine; and (3) it is being developed for chronic use, whereas current CBP products are marketed for two to three weeks of use. We expect that any applications we submit to the Food and Drug Administration, or FDA, for approval of TNX-102 SL will be submitted under Section 505(b)(2) of the Federal Food, Drug, and Cosmetic Act, or FDCA, which we believe will allow for a shorter timeline of clinical and non-clinical development as compared to that needed to fulfill the requirements of Section 505(b)(1), under which new chemical entities, or NCEs, that have never been marketed in the United States, are generally developed to meet the FDA’s requirements for new drug approvals.
We have conducted several clinical and non-clinical pharmacokinetic studies of TNX-102 sublingual formulations, which we believe support the development of TNX-102 SL as a novel therapeutic product for FM and PTSD. Results from these studies demonstrate a number of potentially advantageous characteristics as compared to current CBP-containing products (Flexeril® and Amrix®), which are not approved for these indications. For example, our Phase 1 comparative studies showed that TNX-102 SL results in faster systemic absorption and significantly higher plasma levels of CBP in the first hour following administration relative to oral CBP tablets. TNX-102 SL was generally well-tolerated, with no serious adverse events reported in these studies. Some subjects experienced transient numbness on the tongue after TNX-102 SL administration, and other side-effects reported were similar to those associated with current CBP products.
TNX-102 SL – Fibromyalgia Program
We are developing TNX-102 SL for the treatment of FM under a U.S. Investigational New Drug application, or IND, and we held an End-of-Phase 2/Pre-Phase 3 meeting with the FDA in February 2013. TNX-102 SL is currently in a Phase 2b/3 clinical trial for the improvement of pain in subjects with FM, from which we expect to report initial results in the fourth quarter of 2014. Our therapeutic strategy is supported by results from a randomized, double-blind, placebo-controlled Phase 2a study of low dose TNX-102 immediate release capsules, or TNX-102 capsules, which we have also referred to as VLD CBP, taken between dinner and bedtime in 36 subjects with FM, which demonstrated a significant decrease in pain and other symptoms after eight weeks of treatment. This study also demonstrated that TNX-102 capsules led to a significant improvement in objective measures of sleep quality, which we believe relates to the mechanism by which CBP leads to improvement of FM symptoms. We have completed four Phase 1 studies under Canadian Clinical Trial Applications. Our Phase 1 studies demonstrated TNX-102 SL to exhibit a pharmacokinetic profile that we believe supports chronic bedtime administration for the treatment of FM, and is distinct from those of currently-available CBP products.
FM is a chronic syndrome characterized by widespread musculoskeletal pain accompanied by fatigue, sleep, memory and mood issues. According to the National Institutes of Health, there are approximately five million people suffering from FM in the U.S. The peak incidence of FM occurs at 20 – 50 years of age, and 80-90% of diagnosed patients are female. FM may have a substantial negative impact on social and occupational function, including disrupted relationships with family and friends, social isolation, reduced activities of daily living and leisure activities, avoidance of physical activity, and loss of career or inability to advance in careers or education.
Although the disordered brain processes that underlie FM are yet to be fully understood, the mechanisms of drugs that treat central pain are believed to target certain aspects of nerve signaling. Three drugs, Lyrica® (pregabalin), Cymbalta® (duloxetine), and Savella® (milnacipran), are approved by the FDA for the management of FM and are believed to act upon molecular pathways involved in central pain. Lyrica is believed to affect nerve signaling by blocking calcium channels on nerve cells, and is considered a nerve membrane stabilizer. Cymbalta and Savella are believed to directly inhibit the reuptake of serotonin and norepinephrine by nerves, and are referred to as Serotonin and Norepinephrine Reuptake Inhibitors, or SNRIs. CBP, the active ingredient of TNX-102 SL, is a selective antagonist of serotonin and norepinephrine receptors as well as an inhibitor of serotonin and norepinephrine reuptake, and we refer to it as a Serotonin and Norepinephrine receptor Antagonist and Reuptake Inhibitor, or SNARI.
As many products used for the treatment of FM are approved and marketed for other conditions, sales of these products related specifically to FM can only be estimated. Based on information obtained from publicly available sources, we believe U.S. sales of prescription drugs specifically for the treatment of FM totaled approximately $1.5 billion in 2012, and we believe this segment had grown at a compounded annual growth rate of approximately 14% between 2007 and 2012. Based on information obtained from publicly available sources, we believe 2012 sales of Cymbalta, Lyrica, and Savella in FM were approximately $600 million, $475 million, and $100 million, respectively.
Despite the availability and use of a variety of pharmacologic and non-pharmacologic interventions, FM remains a significant unmet medical need. Many patients fail to adequately respond to the approved medications, or discontinue therapy due to poor tolerability. Prescription pain and sleep medications are frequently taken ‘off-label’ for symptomatic relief, despite the lack of evidence that such medications provide a meaningful or durable therapeutic effect. An important goal of FM treatment is to reduce the dependence on opiate analgesic as well as on benzodiazepine and non-benzodiazepine sedative-hypnotic medications by FM patients. Since CBP has no recognized addictive potential, we believe that TNX-102 SL, if approved, could reduce the exposure of FM patients to medications that have not been shown to be effective in treating FM and are associated with significant safety risks.
At our End-of-Phase 2/Pre-Phase 3 meeting with the FDA, we discussed the design of our clinical program, including the acceptability of the pivotal study design and the proposed registration plan, to support the approval of TNX-102 SL for the management of FM. We believe that positive results from two adequate, well-controlled safety and efficacy studies and the establishment of long-term safety for chronic use would support the approval of TNX-102 SL for the management of FM.
Phase 2b/3 “BESTFIT” Study
We are currently conducting the randomized, double-blind, placebo-controlled Phase 2b/3 BEdtime Sublingual TNX-102 SL as Fibromyalgia Intervention Therapy (BESTFIT) trial, which we initiated in September 2013 under the IND. In this multicenter clinical trial, subjects with FM are treated with either TNX-102 2.8 mg sublingual tablets (SL) or a placebo at bedtime daily for 12 weeks. We expect to enroll approximately 200 patients into this study. The primary efficacy endpoint is change in pain from baseline to week 12. If successful, this trial will serve as the first of two pivotal studies to support an NDA for TNX-102 SL in FM. We have engaged Premier Research International, LLC, a contract research organization, or CRO, to provide clinical and data management services for this Phase 2b/3 trial. We expect to report initial efficacy results from the BESTFIT trial in the fourth quarter of 2014.
The primary efficacy measure in this study will be the change in pain severity at week 12 with TNX-102 SL as compared to placebo, as assessed by the Numeric Rating Scale, or NRS. This endpoint is similar to that utilized in clinical trials of drug products currently approved for use in FM. We are also collecting information on other outcome measures, including NRS scores at other time points, the revised Fibromyalgia Impact Questionnaire, and the Patient Global Impression of Change.
Long-Term Safety Exposure Study
In December 2013, we announced the initiation of F203, a 12-month open-label extension study of TNX-102 SL to be taken daily at bedtime, into which patients who have completed the BESTFIT study may enroll. The goal is to obtain sufficient 6 and 12 month exposure data in FM patients to meet the NDA submission requirement.
TNX-102 SL – Post-Traumatic Stress Disorder Program
We are also advancing TNX-102 SL for the management of PTSD. We held a pre-IND meeting with the FDA in October 2012, and we plan to file an IND to pursue this indication in the second quarter of 2014. We plan to begin a Proof-of-Concept (POC) trial of TNX-102 SL in subjects with military-related PTSD in the third quarter of 2014. Based on the results of the POC trial, we will meet with the FDA to finalize the design of the registration studies to support the PTSD NDA. We believe the approval will be based upon positive results from two adequate, well-controlled efficacy and safety studies and long-term (6 and 12 month) safety exposure data. We expect the long-term safety exposure data generated by our clinical development of TNX-102 SL in FM can be used to support the PTSD indication.
TNX-201 – Episodic Tension-Type Headache Program
TNX-201 is a single isomer of isometheptene mucate (IMH) and is under development as a treatment for ETTH, an indication believed to affect approximately 20% of the global adult population. Although currently not approved for any indication, IMH has an extensive history of use as a prescription pharmaceutical in the U.S. as a mixture of two mirror-image isomers, also known as a racemic mixture. Racemic IMH has been marketed in combination products for the relief of tension and vascular headaches (examples include Midrin® and MigraTen®). The selection of a single isomer of IMH for development may confer an improved clinical profile as compared to the racemic mixture, consistent with the FDA Stereoisomeric Drugs Development Policy, and is supported by our pharmacology data. We held a pre-IND meeting with the FDA in January 2014 to discuss the regulatory pathway for the development of TNX-201 for the treatment of ETTH. The initial IND for TNX-201 will not require any additional nonclinical data to support a first-in-man study, and we plan to conduct a Phase I comparative pharmacokinetic and safety study in the fourth quarter of 2014. Although the development of TNX-201 will be based on the available information on racemic IMH, the NDA approval will be required to conform with the 505(b)(1) NDA requirement.
Additional Product Candidates
In addition to TNX-102 SL, we have developed other innovative formulations of CBP, including TNX-102 promicellar gelatin capsule, or TNX-102 gelcap. We have developed TNX-102 gelcap under an agreement with Lipocine, Inc., or Lipocine, a contract formulation developer and small-scale manufacturer. We met with the FDA to discuss the TNX-102 gelcap development program in August 2011 and have generated clinical data that support the further development of this candidate. However, we currently do not plan to advance TNX-102 gelcap, and in March 2014, we notified Lipocine of our decision to not exercise our option to license Lipocine’s technology, although we own all the work product, information and data from the studies conducted.
We also have a pipeline of other product candidates, including TNX-301. TNX-301 is a fixed dose combination of two FDA-approved drugs, disulfiram and selegiline. We intend to develop TNX-301 under the 505(b)(2) provision as a treatment for alcohol abuse and dependence, and plan to begin formulation work on TNX-301 in 2014. In addition, we recently acquired rights to intellectual property on the development of protective agents against radiation exposure and on the development of novel smallpox vaccines. The radio- and chemo-protective technology relates to proprietary forms of a small molecular pharmaceutical agent, which is believed to protect against ionizing radiation after oral administration. The smallpox vaccine technology relates to proprietary forms of live vaccinia vaccines which may be safer than ACAM2000, which is the only currently available replication competent, live vaccinia vaccine to protect against smallpox disease. As we interact with the United States Department of Defense and related biodefense agencies regarding our development of TNX-102 SL for PTSD, we believe these technologies will expand our interaction and cooperation with such agencies. We plan to perform non-clinical research and development on these programs in 2014.
For competitive reasons, we typically do not disclose the identities of the active ingredients or targeted indications in our pipeline until a U.S. patent has been allowed or issued.
Our Strategy
Our objective is to develop and commercialize our product candidates to treat CNS conditions, including FM, PTSD and ETTH. The principal components of our strategy to achieve this objective are to:
|
|
· |
adopt a multi-pronged patent strategy to protect our products, including patents that protect methods of use for the active ingredients in our products, the formulation technology employed in our products, the performance characteristics of our products in the human body and the composition-of-matter of our products;
|
|
|
· |
provide clear value propositions to third-party payers, including managed care companies or government programs such as Medicare, to merit reimbursement for our product candidates; and |
|
|
· |
establish and maintain a sales and marketing infrastructure, such that we will be able to effectively commercialize our products once approved. |
Pursue development and regulatory approval pathways. We are developing TNX-102 SL under the Section 505(b)(2) FDA pathway. This pathway can reduce the time and expense required for our development programs by allowing our use of previously-generated safety and efficacy information regarding the active pharmaceutical ingredients in our lead product candidates to support the filing and approval of our NDA application. Our use of this information may help reduce the size and scope of our preclinical and clinical trials. We expect to develop TNX-201 under Section 505(b)(1), the pathway followed for an NCE or marketed drug without an approved NDA in the United States. For TNX-201, a single isomer of a marketed racemic drug, we are able to leverage the existing racemic IMH human experience to design an efficient development program. While we expect to pursue the development of TNX-301 under Section 505(b)(2), we have not yet discussed this candidate with the FDA. In general, our ability to pursue the 505(b)(1) or 505(b)(2) regulatory pathways will depend, at least in part, on the data available for reference of the particular candidate to support product registration. The use of a drug product for the treatment of a condition other than one of its approved label indications is called off-label use. The development of an existing FDA-approved drug for the treatment of a condition other than one of its approved label indications is considered a “new use”. For companies involved in the ethical development and marketing of prescription drugs in the US, FDA approval of a new use or new label indication is the only legal basis of marketing claims for that use or indication. Off-label use is not recognized by the FDA or FDA-regulated companies as a new use.
Adopt a multi-pronged patent strategy. We are pursuing a multi-pronged patent strategy by seeking intellectual property protection on several aspects of our products. Aspects we seek to protect include, among others, methods of use for certain known active pharmaceutical ingredients, formulation technologies incorporated into our products, performance characteristics of our products in the human body and the composition-of-matter of our products. With respect to methods of use patents, we believe the therapeutic uses we target are new uses for these active ingredients and we have been issued patents directed to certain aspects of our new uses. For example, the invention of bedtime TNX-102 as a treatment for FM was novel and unexpected when our patents were filed in 2000. We are seeking additional patents to cover other new uses. For example, we filed a patent application seeking to protect the use of CBP in PTSD. With respect to formulation patents, we believe our products will be protected by patents that describe inventions of technology for making new formulations, which may include novel routes of delivery for the active ingredients. With respect to patents related to the performance characteristics of our products in the human body, we believe our products will be protected by patents that describe novel pharmacokinetic properties of the active ingredient, as well as of its active metabolites, at certain times after administration. For example, we filed a patent application seeking to protect novel pharmacokinetic properties of CBP as enabled by TNX-102 SL. In the case of TNX-201, for which the active ingredient is a single isomer of racemic isometheptene, we have filed a patent application seeking to protect the composition-of-matter of oral dosage forms that contain only the single isomer and not the racemic mixture.
Provide clear value propositions to third-party payors to merit reimbursement for our product candidates. We are designing our clinical development programs to demonstrate compelling competitive advantages to patients and prescribers and also to demonstrate value propositions to third-party payors. We believe TNX-102 SL might help in the management of FM by reducing pain and other symptoms, such as fatigue. In addition, primarily as a result of its lower dosage, we believe that bedtime treatment with TNX-102 SL will have fewer day time side-effects than off-label bedtime treatment with immediate-release CBP products approved for the treatment of muscle spasm, or CBP IR. For FM, we believe an FDA-approved product would capture some of the off-label use of CBP IR. Because FDA approvals are based on objective data, we believe that third-party payors will provide reimbursement for an FDA approved product, even at a premium price relative to other drugs that are used off-label, such as CBP IR, tizanidine, baclofen, carisoprodol or metaxalone. For example, third-party payors reimburse the use of Lyrica, Cymbalta and Savella for FM despite the availability of off-label generic versions of drugs with similar mechanisms of action, for example, Neurontin® (gabapentin) and generic anti-depressants, respectively. Cymbalta lost its U.S. patent exclusivity in December 2013.
Establish and maintain an effective sales and marketing infrastructure. We believe TNX-102 SL and TNX-201 can be marketed to physicians in the United States by means of a sales force built by or engaged by us. Many large and small pharmaceutical companies engage contract sales organizations, or CSOs, to launch products and contracts with such organizations can be structured as a “rent-to-buy” model. The flexibility and scalability of such organizations has made it possible for many emerging companies to decide to market their own products. Therefore, we plan to work with CSOs to develop the capabilities of building a sales force, initially through contracting, and we may eventually internalize the sales and marketing capabilities. Another option for certain of our drug development candidates, including TNX-102 SL and TNX-201, would be to partner with companies that already have significant marketing capabilities in the same, or similar, therapeutic areas. If we determine that such a strategy would be more favorable than developing our own sales capabilities, we would seek to enter into collaborations with pharmaceutical or biotechnology companies for the commercialization of our products.
Our Lead Product Candidate
Our lead product candidate is TNX-102 SL, which we are developing for the treatment of FM and PTSD. TNX-102 SL consists of CBP in a mixture of inactive ingredients that are called “excipients”, which we believe will improve the absorption rate of CBP in ways that will optimize the product for bedtime treatment. The excipients used in TNX-102 SL are approved by the FDA for pharmaceutical uses.
Cyclobenzaprine
CBP was first synthesized in 1961 by Merck, and the 10 mg Flexeril immediate-release, or IR, dose form was FDA approved in 1977 for the relief of muscle spasm associated with acute, painful musculoskeletal conditions as an adjunct to rest and physical therapy.
Although a number of clinical studies have addressed the potential use and benefit of CBP in treating symptoms of FM, to our knowledge these studies have not motivated a sponsor to pursue FDA approval.
Based on CBP’s safety and efficacy for treating muscle spasm, in the 1990s, Merck conducted studies to support an application to market a 5 mg Flexeril tablet for the over-the-counter, or OTC, market, whereby patients can purchase medicine without a physician’s prescription. Although Merck’s studies re-affirmed the safety and demonstrated efficacy of 5 mg Flexeril in several large trials, the OTC division of the FDA rejected the application for use without a prescription, apparently, we believe, because muscle spasm was deemed a condition that required a physician to diagnose and supervise treatment.
Merck divested the Flexeril franchise to Alza Pharmaceuticals, or Alza, which was subsequently acquired by Johnson and Johnson and Flexeril is part of its McNeil Consumer Healthcare division, or McNeil. Based largely on the Merck studies, McNeil won approval of Flexeril 5 mg tablets as a prescription medicine to treat muscle spasm. McNeil promoted Flexeril 5 mg tablets for the three year period of market exclusivity based on The Drug Price Competition and Patent Term Restoration Act of 1984, generally referred to as the Hatch-Waxman Act. Following this exclusivity period, several generics entered the market and took market share from Flexeril. McNeil has discontinued the manufacture of Flexeril.
Despite the approved uses of CBP in treating muscle spasm, we believe current marketed formulations of CBP are limited for treating FM by slow and unpredictable absorption. Following the ingestion of CBP IR, it takes more than one hour for clinically-meaningful blood levels to be achieved. As described in the Flexeril package insert, the amount of CBP absorbed into the bloodstream varies between 33 – 55% of the dose ingested. The variability in absorption may be due to several factors, including effects of the stomach pH (acidity or base) on the dissolution of the tablets, as well as the context of either an empty stomach or a recent meal. Food in the stomach and small intestine from a recent meal contributes to variability in absorbing other drugs. The uncertainties in absorption rates make it challenging for a physician contemplating a bedtime treatment for FM to ensure the intended therapeutic effect is achieved without risking side effects like next-day drowsiness, which could result if the patient has too much CBP remaining in the bloodstream the next day.
If a product could provide rapid and consistent absorption of CBP, patients would be more likely to receive a drug exposure profile that is aligned with the intended period of exposure and less likely to receive too little drug to receive a therapeutic effect. Conversely, patients would be less likely to receive too much drug, which might lead to potential side effects, including next-day drowsiness. An optimal bedtime CBP product could have faster absorption, lower blood levels in the morning and more predictable effects than the IR tablet format. We have tested a number of technologies to optimize the properties of CBP as a bedtime therapy for FM and PTSD. Our lead product, TNX-102 SL is a novel sublingual tablet form of CBP that we have tested in pre-clinical and clinical studies. We entered TNX-102 SL into a potential pivotal clinical trial in FM in September 2013, and we plan to begin a POC trial in PTSD in the third quarter of 2014. We believe the unique properties of TNX-102 SL, as demonstrated by the results of our studies, support its development in both FM and PTSD.
TNX-102 SL in Fibromyalgia Syndrome
TNX-102 SL, our lead product candidate, is a rapidly disintegrating tablet containing CBP that is designed to be placed under the tongue at bedtime. The development of TNX-102 SL in FM is supported by the results of the Moldofsky Study, which evaluated oral administration of TNX-102 capsules in the evening, as well as by preclinical and comparative clinical pharmacokinetic studies.
In the Moldofsky Study, which was a randomized, double-blind, placebo-controlled, Phase 2a trial, it was demonstrated that TNX-102 capsules, swallowed between dinner and bedtime, resulted in significant decreases in next-day pain and other core FM symptoms after eight weeks of treatment, as well as in a significant improvement in sleep quality. We believe that CBP exerts its benefit in FM via its ability to improve the restorative quality of sleep, which has been shown to be frequently impaired in patients with FM. Current CBP products are believed to be widely used off-label by FM patients.
FM is diagnosed by groups of symptoms that have been defined by committees of the American College of Rheumatology, or ACR, and a committee of experts from the organization Outcome Measures in Rheumatology. In 2007, Pfizer’s Lyrica became the first medicine approved by the FDA for the management of FM. In 2008, Eli Lilly’s Cymbalta became the second medicine approved by the FDA for the management of FM. In 2009, Savella was the third medicine approved by the FDA for the management of FM. Savella is marketed by Forest Laboratories.
Product Development Plan
Phase 2a Data of TNX-102 capsules in FM Patients
Our motivation to focus our efforts on developing TNX-102 SL for FM stems from the results of the Moldofsky Study, the related rights to which we acquired from L&L. Specifically, this study was a randomized, double-blind, placebo-controlled, dose-escalating eight week trial conducted at two study centers. The study randomized 36 subjects, all of whom met ACR criteria for FM.
Patients received TNX-102 capsules or placebo to ingest after dinner and before bedtime. Each TNX-102 capsule contained 1 mg of CBP. Initially, patients took one capsule each evening, but over the course of the study, they were allowed to increase the number of capsules taken, up to four per evening.
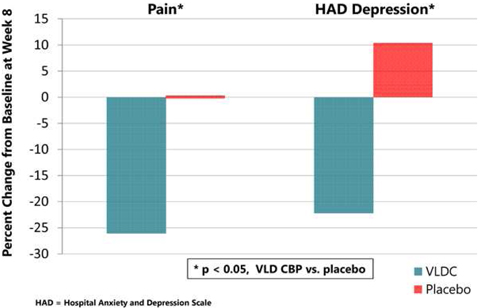
At week eight, patients treated with TNX-102 capsules demonstrated significant improvements in pain, fatigue and tenderness relative to baseline, whereas placebo-treated patients did not improve. Although this study excluded patients who met formal criteria for major depressive disorder or any anxiety disorder, there is a high degree of co-existing symptoms of depression and anxiety associated with FM. Relative to baseline, treatment with TNX-102 capsules also resulted in a significant reduction in total Hospital Anxiety and Depression Scale score, which measures symptoms of anxiety and depression, and the HAD depression subscore which measures depressive symptoms.
Figure 1: Results of a Phase 2a Study of TNX-102 capsules in FM patients as administered between dinner and bedtime.
As illustrated in Figure 1, this study showed that treatment with TNX-102 capsules as compared to treatment with placebo:
|
|
· |
decreased musculoskeletal pain, by demonstrating a significant decrease in mean subject-assessed numeric pain score (p<0.05); and |
|
|
· |
improved mood, by demonstrating a significant decrease in mean HAD depression subscore (p<0.05). |
This study also showed that TNX-102 capsules taken between dinner and bedtime resulted in a significant improvement in objective measures of sleep quality. We believe that CBP exerts its benefit in FM via its ability to improve the restorative quality of sleep, which has been shown to be frequently impaired in patients with FM.
In this study, TNX-102 capsules were well tolerated, with no serious adverse events or discontinuations due to adverse events.
This research was published in the Journal of Rheumatology, in an article entitled “Effects of Bedtime Very Low Dose (VLD) Cyclobenzaprine (CBP) on Symptoms and Sleep Physiology in Patients with Fibromyalgia Syndrome (FM): A Double-blind, Randomized, Placebo-controlled Study.” The citation is: Moldofsky H, Harris H, Kwong T, Archambault WT and Lederman S. J Rheum 2011 Dec;38(12):2653-63.
Pharmacokinetic and Bioavailability Studies
We have conducted preclinical and clinical studies of our sublingual formulations of CBP, which have evaluated the pharmacokinetics of these formulations as well as their comparative bioavailability to oral CBP.
Our preclinical and clinical studies demonstrated that our sublingual formulations provide faster delivery and more efficient systemic absorption of CBP as compared to current oral forms of the drug.
In three Phase I comparative pharmacokinetic and bioavailability studies, TNX-102 SL was generally well tolerated. There were no unexpected adverse events, with the exception of a mild, temporary numbness at the tongue experienced by less than one-third of the subjects that received TNX-102 SL tablets.
Phase 2b/3 “BESTFIT” Study
We are currently conducting a Phase 2b/3 study of TNX-102 SL in FM called the BESTFIT trial. In this multicenter, randomized, double-blind, placebo-controlled clinical trial, FM patients will be administered either TNX-102 SL or placebo at bedtime nightly for 12 weeks. We expect that our BESTFIT trial, if successful and accepted by the FDA, will be one of the two pivotal studies required to support the NDA approval. The study began in September 2013 and we expect to announce initial results in the fourth quarter of 2014.
Long-Term Safety Exposure Study
In December 2013, we announced the initiation of F203, a 12-month open-label extension study of TNX-102 SL to be taken daily at bedtime, into which patients who have completed the BESTFIT study may enroll. The goal is to obtain sufficient 6 and 12 month safety exposure data in FM patients to meet the NDA submission requirement.
Prospective Confirmatory Phase 3 Study
If our Phase 2b/3 BESTFIT study of TNX-102 SL in FM is successful, then we expect to conduct a 12-week, randomized, double-blind, placebo-controlled confirmatory Phase 3 study of TNX-102 SL in support of product registration. It is likely that the primary efficacy measure in this study will be the change in pain severity with TNX-102 SL as compared to a placebo at week 12, as assessed by the NRS, similar to the primary efficacy measure of BESTFIT. Secondary outcome measures will be determined based on the results from the BESTFIT study. These will be carefully selected to support competitive labeling for TNX-102 SL for FM.
Prospective Multi-dose Pharmacokinetic Study
Since CBP will be used chronically in TNX-102 SL, we plan to study TNX-102 SL in comparison to CBP IR in a multiple-day dosing (once daily) study. The results of this study will provide information regarding blood levels of CBP resulting from use of the marketed IR tablet and our sublingual TNX-102 SL tablet when taken in a multiple day regimen. We expect the data from this study to serve as a ‘bridge’, in that they will allow us to use the CBP IR tablet as the reference product in our submission of a Section 505(b)(2) NDA for TNX-102 SL.
Prospective Study Comparing Safety and Tolerability of TNX-102 SL with CBP IR
We plan to conduct a small study designed to evaluate next morning drowsiness and other cognitive measures following the bedtime use of TNX-102 SL and the bedtime use of CBP IR. The goal of this study is to determine the potential benefit of TNX-102 SL compared with CBP IR on next morning drowsiness and on other cognitive functions.
Nonclinical
In addition to the clinical data necessary to support the TNX-102 SL 505(b)(2) NDA filing for the fibromyalgia indication, the FDA also clarified the nonclinical studies required for the NDA filing since the information from the reference product is either unavailable for reference or failed to meet the current regulatory standard. In 2014, we will be selecting an FDA-certified Good Laboratory Practices laboratory to conduct a six month repeated-dose toxicology study in rats, a nine month repeated-dose toxicology study in dogs and a peri- and post-natal Segment III study required for the NDA filing. We plan to submit these draft toxicology protocols for FDA review and seek agreement on the doses and facilities chosen for these studies. These studies will be performed concurrently with the Phase 3 study and will be completed ahead of the NDA submission. Based on the Flexeril labeling and post-marketing surveillance information, there is no evidence of abuse for CBP. As a result, we will not have to assess the abuse potential of TNX-102 SL for the NDA submission.
Manufacturing
The TNX-102 SL drug product that has been manufactured for our BESTFIT study was manufactured in a small-scale current Good Manufacturing Practice, or cGMP, facility that is licensed to manufacture clinical trial materials, but not equipped for large-scale commercial production. For the second pivotal study and for the commercial product, we have engaged a commercial cGMP facility that is capable of manufacturing the registration batches to support the NDA. The product’s comparability will be supported by the bioequivalence results from the “bridging” study, TNX-CY-F105.
Other NDA Requirements
We have submitted a Pediatric Study Plan, or PSP, which contains a partial waiver of the requirement to submit pediatric assessments per Section 505B(a)(4)(A)(i) of the FDCA. Final PSP requirement will be determined at the time of NDA approval.
Based our discussions with the FDA and the FDA formal meeting minutes, we will not have to conduct special populations (geriatric and renal/hepatic impaired), drug-drug interaction or a cardiovascular safety study to support the NDA filing. Due to the well-established safety profile of CBP at much higher doses than we proposed for FM, the FDA requests no risk management plan or medication guide for this product.
Regulatory Strategy
The FDA approvals of Lyrica, Cymbalta and Savella establish a regulatory approval standard for the management of FM. However, given the heterogeneity of patients with this disease, it may not prove to be the only pathway or approval requirement. We hope to register TNX-102 SL with the FDA through the provisions of Section 505(b)(2). This regulatory pathway may help to accelerate product development and reduce overall business risk. The 505(b)(2)-based product development plan for TNX-102 SL is designed to leverage the safety data that have been generated by other manufacturers for CBP-containing products and accepted by the FDA in support of their product registrations, in addition to the safety data we generate. TNX-102 SL contains significantly less active CBP than other marketed products. We believe that the safety data package from these products and the CBP prescriptions utilization database analyzed by IMS Health Incorporated will provide adequate safety margin to support TNX-102 SL development. At our End-of-Phase 2/Pre-Phase 3 meeting we held with the FDA in February 2013, we discussed the nature and extent of the Phase 2b and Phase 3 clinical trials we need to conduct to so as to receive regulatory acceptance of our proposed NDA plan for a differentiated product for the management of FM.
If NDA approval of TNX-102 SL is granted, in addition to the three-year marketing exclusivity provided by law, we expect this product to be protected by patents that extend through at least 2021, during which time it should not be subject to generic substitution. We plan to continue to support the TNX-102 SL program with new patent applications as we obtain data from the clinical evaluation of our new formulation in healthy human subjects and in FM patients. For example, we have recently filed patent applications on TNX-102 SL which, if issued, would be expected to provide protection from generic substitution until at least 2033.
TNX-102 SL in Post-Traumatic Stress Disorder
We are also developing TNX-102 SL for the management of PTSD, a psychiatric disorder that begins in the aftermath of traumatic experiences. We held a pre-IND meeting with the FDA in October 2012, at which our clinical program for PTSD was discussed. We plan to file an IND in the second quarter of 2014 to support the initiation of a POC efficacy study in the third quarter of 2014.
Parallels Between FM and PTSD
A number of parallels have been noted between FM and PTSD. In addition, symptom overlap may exist between patients diagnosed with FM or PTSD. In a survey of males with PTSD or major depression (Amital et al, Posttraumatic stress disorder, tenderness, and fibromyalgia syndrome: are they different entities? J. Psychosom. Res. 2006, 61(5):663-9), 49% of PTSD patients met the ACR criteria for FM compared to 5% of major depression patients. Conversely, in a different survey of FM patients (Cohen et al., Prevalence of post-traumatic stress disorder in fibromyalgia patients: overlapping syndromes or post-traumatic fibromyalgia syndrome? Semin. Arthritis Rheum. 2002, 32(1):38-50), 57% of the sample had symptoms associated with PTSD.
A core feature of PTSD is sleep disturbance, including insomnia and nightmares. Sleep disturbances are believed to exacerbate daytime symptoms of PTSD, including irritability, poor concentration, and diminished interest in significant activities. We believe the sleep disturbances of PTSD bear similarity to those associated with FM.
Emerging Market Opportunity
The selective serotonin reuptake inhibitors Paxil® (paroxetine) and Zoloft® (sertraline) are FDA approved for PTSD, but are not satisfactory treatments for many patients. Other drugs that show promise for the treatment of PTSD, but are not FDA approved, include antidepressants such as nefazodone, mirtazapine and trazodone; the antihistamine cyproheptadine; certain atypical antipsychotics such as olanzapine and risperidone; and an adrenergic alpha-1 receptor blocker, prazosin. Prazosin may decrease nightmares and insomnia and has been associated with improvements in daytime PTSD symptoms, depression, and quality of life.
Our rationale for studying the effects of CBP in PTSD derives from the following:
|
|
· |
our clinical studies that treatment with TNX-102 capsules improves FM symptoms, a disorder having significant overlap with PTSD; |
|
|
· |
our clinical studies that TNX-102 capsules can improve sleep quality, which is impaired in PTSD; and |
|
|
· |
in receptor binding studies conducted by Caliper under our direction, CBP interacts with a receptor on brain cells called the serotonin type 2a receptor. Based on numerous peer-reviewed scientific publications, we have identified a number of compounds that bind this receptor that have been shown to have effects in treating PTSD. Therefore, it is our belief that CBP, because it binds to the serotonin type 2a receptor, will have a therapeutic effect in treating PTSD. |
As very little information was available on the biochemical effects of CBP and its primary metabolite, norcyclobenzaprine, or nCBP, in the central nervous system, we have engaged several CROs to better understand the interactions of these agents with certain receptors in the brain. CROs we have engaged in this effort include Caliper, Cerep, Millipore, and DiscoveRx. Results from a series of binding and functional studies show that both of these molecules are potent antagonists of the serotonin type 2a and the histamine H1 receptors, which known to have effects on sleep and sleep maintenance. The results also show that CBP and nCBP antagonize the adrenergic alpha 1A and 1B receptors, which may have effects on autonomic dysfunction. The results of some of these studies were presented at a poster session during the 2012 American College of Rheumatology Annual Meeting (Daugherty et al, “Cyclobenzaprine (CBP) and its Major Metabolite Norcyclobenzaprine (nCBP) are Potent Antagonists of Human Serotonin Receptor 2a (5-HT2a), Histamine Receptor H1 and Alpha-Adrenergic Receptors: Mechanistic and Safety Implications for Treating Fibromyalgia Syndrome by Improving Sleep Quality”, Abstract #960).
Product Development Path
Based on the recommendations and guidance received at our October 2012 pre-IND meeting with the FDA and in consultation with experts in this psychiatric disorder, we plan to file an IND application for TNX-102 SL in the PTSD indication in the second quarter of 2014, and to begin a POC trial in the third quarter of 2014. We expect to be able to use TNX-102 SL tablets manufactured for the FM studies in this clinical trial.
Prospective Proof-of-Concept Study
The IND to be filed in the second quarter of 2014 will have the information necessary to support a POC clinical study to ascertain the potential efficacy of TNX-102 SL in PTSD. We expect this will be a randomized, double-blind, placebo-controlled, parallel study of bedtime TNX-102 SL in military-related PTSD subjects. We expect the dosing period to be six weeks, and the primary efficacy measure to be the change in the Clinician-Administered PTSD Scale from baseline to week six.
Prospective Phase 3 Studies
If our POC trial of TNX-102 SL in PTSD is successful, we will meet with the FDA to finalize the design of the registration studies to support the PTSD NDA. We believe the approval will be comprised of positive results from two adequate, well-controlled efficacy and safety studies and long-term (6 and 12 month) safety exposure data. We expect the long-term safety exposure data generated by our clinical development of TNX-102 SL in FM can be used to support the PTSD indication.
Regulatory Strategy
The approvals by the FDA of Paxil (paroxetine) and Zoloft (sertraline) for treating PTSD established a regulatory approval pathway for symptom reduction in PTSD. We believe our clinical development program of TNX-102 SL and the long term safety data generated from the TNX-102 SL FM NDA program will result in a differentiated product suitable for chronic use for the treatment of PTSD. We believe that our planned clinical trials in PTSD, if successful, will provide sufficient evidence of clinical efficacy and safety to support a 505(b)(2) NDA for TNX-102 SL for the management of PTSD.
We held a pre-IND meeting with the FDA on TNX-102 SL in PTSD in October 2012, and we expect to file an IND in the second quarter of 2014 and to initiate a POC study in the third quarter of 2014. We plan to meet with the FDA when we complete the POC efficacy study to further discuss the development plan, especially the design of the pivotal studies. If the results from the POC efficacy study are positive, we plan to seek a Breakthrough Therapy designation for TNX-102 SL in PTSD. The Breakthrough Therapy designation process is a new and uncertain process, in which the majority of requests for designation have been denied.
Drug Delivery Technology
TNX-102 SL
TNX-102 SL is a small tablet that rapidly disintegrates in saliva and delivers CBP across the mucosal membrane into the systemic circulation. In addition to CBP, TNX-102 SL contains excipients, which are well-characterized, are listed in the Inactive Ingredient Guide and are approved for pharmaceutical use. TNX-102 SL contains sublingual absorption-enabling ingredients that promote a local oral environment that facilitates mucosal absorption of CBP. These include agents that favor a mildly basic salivary pH. We own all rights to TNX-102 SL in all geographies, and we bear no obligations to third-parties for any future development or commercialization.
TNX-102 Gelcap
In June 2007, we entered into a Feasibility and Option Agreement with Lipocine, which was amended in October 2010 (the “Feasibility Agreement”). Pursuant to the Feasibility Agreement, we identified and obtained an exclusive worldwide option on technology from Lipocine that employs mixtures of different types of lipids to envelop CBP molecules in the small intestine and facilitate absorption into the bloodstream. We selected a candidate formulation, TNX-102 gelcap, based on properties that included the dispersion of CBP in simulated gastric or small-intestinal fluids and the stability of the formulation over time. Lipocine was also engaged to manufacture gelatin capsules of TNX-102 gelcap for use in a pharmacokinetic trial, for which we reported results in April 2012. In March 2014, we completed the final report of the pharmacokinetic trial (the “Final Report”) and had 30 days to decide whether to exercise the option to license certain technology owned by Lipocine. Following our receipt of the Final Report, in March 2014, we notified Lipocine of our decision to not exercise the option, although we own all the work product, information and data from the studies conducted.
Market Dynamics
We believe the U.S. market for products that treat CNS conditions has several characteristics that make it an attractive market for pharmaceuticals, including that the customer base is driven by physicians who are involved in long-term care of patients with chronic disorders. Patients with CNS disorders sometimes carry disease burdens that require long-term treatment.
We believe the market for FDA-approved FM treatments is underserved and that there is a constant need for new treatment options, since many prescription drugs provide relief only to some of the affected patients, only to some of some patients’ symptoms, or provide relief only for limited periods of time.
In 2007, Lyrica became the first medicine approved by the FDA for the management of FM. Lyrica previously had been approved and marketed to treat pain in other conditions as well as epilepsy. In 2008, Cymbalta became the second medicine approved by the FDA for the management of FM. Cymbalta previously had been approved and marketed to treat depression. FM shares a number of symptoms with depression, and a number of FM patients are believed to experience depression as a co-existing condition. Savella was the third medicine approved by the FDA for the management of FM. Savella’s active ingredient, milnacipran, is approved for the treatment of depression in Europe.
As many products used for the treatment of FM are approved and marketed for other conditions, sales of these products related specifically to FM can only be estimated. Based on information obtained from publicly available sources, we believe U.S. sales of prescription drugs specifically for the treatment of FM totaled approximately $1.5 billion in 2012, and we believe this segment had grown at a compounded annual growth rate of approximately 14% in 2007 – 12. Based on information obtained from publicly available sources, we believe 2012 sales of Cymbalta, Lyrica, and Savella were approximately $600 million, $475 million, and $100 million, respectively. Cymbalta lost its U.S. patent exclusivity in December 2013. Despite the availability of FDA approved products, we believe the current treatment options for FM continue to leave many patients dissatisfied.
Prior to 2007, the landscape of prescription drugs used to treat FM was characterized by off-label use of generically-available therapies. Drugs that had been prescribed as the primary treatments for FM were approved for other indications, with analgesics, antidepressants, and muscle relaxants among the categories receiving the greatest use by the FM population. Despite the significant FM-related sales growth of the three products approved for FM following their approvals for this indication, according to market research performed by Frost and Sullivan on our behalf, the unit volume of medications prescribed to specifically treat FM had been nearly flat between 2007 and 2010, implying that the sales growth of the approved products was mainly driven by patients switching from off-label, generic medications to on-label, branded medications. In particular, these market dynamics are consistent with the interpretation that Lyrica’s growth in FM was driven by switching from off-label analgesics, and Cymbalta’s and Savella’s growth in FM was driven by switching from off-label anti-depressants. Increasingly, Cymbalta, Savella and Lyrica are recognized as central pain inhibitors and not just treatments for their original indications.
Despite the wide use of muscle relaxants by FM patients, this category lacks a product approved for FM. Demand continues to be satisfied by off-label medicines such as CBP, tizanidine, baclofen, carisoprodol and metaxalone. These muscle relaxants have generic and branded versions. According to Frost and Sullivan, 48 million doses of the Flexeril brand and its associated CBP IR generic products were prescribed off-label for FM in 2010 and accounted for approximately 35% of the daily doses of muscle relaxants prescribed for FM that year. These figures indicate that muscle relaxants in general, and CBP in particular, have been widely adopted in FM despite the lack of an approval for this disorder. As FM patients do not typically experience muscle spasm, we believe that the use of muscle relaxants in FM is off-label from a regulatory perspective and provides therapeutic effects to FM patients that are different from those in treating muscle spasm. Therefore, in FM, CBP acts as a central pain inhibitor and not as a muscle relaxant.
Despite the availability and use of a variety of pharmacologic and non-pharmacologic interventions, FM remains a significant unmet medical need. Many patients fail to adequately respond to the approved medications, or discontinue therapy due to poor tolerability. Prescription pain and sleep medications are often taken ‘off-label’ for symptomatic relief, despite the lack of evidence that such medications provide a meaningful or durable therapeutic effect. An important goal of FM treatment is to reduce the dependence on opiate analgesic as well as on benzodiazepine and non-benzodiazepine sedative-hypnotic medications by FM patients. Since CBP has no recognized addictive potential, we believe that TNX-102 SL, if approved, could reduce the exposure of FM patients to medications that have not been shown to be effective in treating FM and are associated with significant safety risks.
Challenges in the Market for CNS Therapies
Developers of pharmaceutical treatments for syndromes and disorders that affect the CNS face special challenges. In many cases, the causes and exacerbating factors of CNS conditions remain unknown. Frequently, key symptoms are known only by patient reports and cannot be objectively validated or measured. Symptoms like pain, fatigue, disturbed sleep, cognitive/concentration problems or altered mood are characteristics of more than one condition. Often, physicians may not agree that a particular patient is affected by one or another condition or by more than one co-existing conditions.
CNS conditions are typically defined by committees of expert professionals who set criteria based on the presence of several symptoms or groups of symptoms. Sometimes groups of subjective symptoms are insufficient to describe CNS disorders and further refinement of diagnostic categories can be achieved by patient demographics, such as gender, age or concurrent medical processes, such as menopause or adolescence. Many CNS conditions, including syndromes and disorders, have not yet been characterized by laboratory tests, such as blood tests or x-ray imaging. However, laboratory tests are often important to exclude other conditions, such as inflammatory or infectious processes. Consequently, a CNS condition is sometimes called a diagnosis of exclusion because inflammation and infection should typically be ruled out by laboratory tests before applying the criteria of groups of symptoms to diagnose it.
Once a CNS condition is diagnosed, physicians may select from among treatment options based on a patient’s symptoms and history. Some medications improve or relieve only one or another symptom in a condition. Consequently, physicians may prescribe several different medications concurrently to treat individual symptoms or groups of symptoms. A desirable quality for CNS medications is the ability to relieve more than one symptom of a CNS condition. Another desirable quality for CNS medications is safety, particularly if a medicine is safe enough to be used with other medicines concurrently or at different times of the day.
Opportunity for New Treatments of FM
We believe the market for the treatment of FM is underserved, which we believe fuels a need for new therapeutic options. Due to the market acceptance of approved FM treatments Cymbalta, Lyrica and Savella, we believe there will be significant interest in effective and well-tolerated drug treatment options.
We believe that if TNX-102 SL won FDA approval, it would be an appealing option because it is believed to act by a different mechanism of action from the currently approved products, and we expect TNX-102 SL will be recommended for use at bedtime. Lyrica is recommended for twice or three-times daily dosing. Cymbalta was found effective at once-daily or twice-daily dosing and is generally restricted to daytime use and not recommended for bedtime use.
Competition
Our industry is highly competitive and subject to rapid and significant technological change. Our potential competitors include large pharmaceutical and biotechnology companies, specialty pharmaceutical and generic drug companies, academic institutions, government agencies and research institutions. We believe that key competitive factors that will affect the development and commercial success of our product candidates are efficacy, safety, tolerability, reliability, price and reimbursement level. Many of our potential competitors, including many of the organizations named below, have substantially greater financial, technical and human resources than we do and significantly greater experience in the discovery and development of product candidates, obtaining FDA and other regulatory approvals of products and the commercialization of those products. Accordingly, our competitors may be more successful than we may be in obtaining FDA approval for drugs and achieving widespread market acceptance. Our competitors’ drugs may be more effective, or more effectively marketed and sold, than any drug we may commercialize and may render our product candidates obsolete or non-competitive before we can recover the expenses of developing and commercializing any of our product candidates. We anticipate that we will face intense and increasing competition as new drugs enter the market and advanced technologies become available. Further, the development of new treatment methods for the conditions we are targeting could render our drugs non-competitive or obsolete.
The markets for medicines to treat FM, PTSD, ETTH and other CNS conditions are well developed and populated with established drugs marketed by large and small pharmaceutical, biotechnology and generic drug companies. Eli Lilly (Cymbalta), Forest Laboratories (Savella), and Pfizer (Lyrica) market FDA approved drugs for FM. Cymbalta lost its U.S. patent exclusivity in December 2013. GlaxoSmithKline (Paxil) and Pfizer (Zoloft) market FDA approved drugs for PTSD. Paxil and Zoloft lost their U.S. patent exclusivities in 2003 and 2006, respectively. Non-prescription medications used for ETTH include non-steroidal anti-inflammatory drugs, including ibuprofen and naproxen; acetaminophen; and aspirin. Medications prescribed for ETTH include Fiorinal, Fiorinal with Codeine, Fioricet, and their generic equivalents.
As of March 2014, we are aware of several companies developing prescription medications for FM, including Allergan, Chelsea Therapeutics, Meda, Merck, Pfizer, RiboCor and Theravance. Clinical trials in the U.S. are registered with the FDA and reported on the website www.clinicaltrials.gov. Medications that are used off-label for the treatment of FM include:
|
|
· muscle relaxants, such as cyclobenzaprine; |
|
|
· anti-depressants, such as amitriptyline, venlafaxine, and trazodone; |
|
|
· benzodiazepine as well as non-benzodiazepine sedative hypnotics. |
A number of companies are developing prescription medications for PTSD, including AstraZeneca, Biotie, Forest, GlaxoSmithKline, Lundbeck, Marinus Pharmaceuticals, Merck, Nanotherapeutics, Johnson and Johnson, Pfizer, and UCB. Medications that are used off-label for the treatment of PTSD include anti-depressants, such as nefazodone and trazodone; the antihistamine cyproheptadine; and certain atypical antipsychotics, such as olanzapine and risperidone.
A number of companies are developing prescription medications for tension-type headache, including Bayer, GlaxoSmithKline, and Pfizer.
Intellectual Property
We believe that we have an extensive patent portfolio and substantial know-how relating to TNX-102 SL and our other product candidates. Our patent portfolio, described more fully below, includes claims directed to TNX-102 SL compositions and methods of use. As of March 21, 2014, we are either the owner of record of or own the contractual right to five issued U.S. patents and 26 issued non-U.S. patents. We are actively pursuing an additional 13 U.S. patent applications, of which three are provisional and 10 are non-provisional, four international patent applications, and 21 non-U.S. patent applications.
We strive to protect the proprietary technology that we believe is important to our business, including our proprietary technology platform, our product candidates, and our processes. We seek patent protection in the United States and internationally for our products, their methods of use and processes of manufacture, and any other technology to which we have rights, where available and when appropriate. We also rely on trade secrets that may be important to the development of our business.
Our success will depend on 1) the ability to obtain and maintain patent and other proprietary rights in commercially important technology, inventions and know-how related to our business, 2) the validity and enforceability of our patents, 3) the continued confidentiality of our trade secrets, and 4) our ability to operate without infringing the valid and enforceable patents and proprietary rights of third parties. We also rely on continuing technological innovation and in-licensing opportunities to develop and maintain our proprietary position.
We cannot be certain that patents will be granted with respect to any of our pending patent applications or with respect to any patent applications we may own or license in the future, nor can we be certain that any of our existing patents or any patents we may own or license in the future will be useful in protecting our technology. For this and more comprehensive risks related to our intellectual property, please see “Risk Factors — Risks Relating to Our Intellectual Property.”
The term of individual patents depends upon the legal term of the patents in the countries in which they are obtained. In most countries in which we file, the patent term is 20 years from the date of filing the first non-provisional priority application. In the United States, a patent’s term may be lengthened by patent term adjustment, which compensates a patentee for administrative delays by the U.S. Patent and Trademark Office, or PTO, in granting a patent, or may be shortened if a patent is terminally disclaimed over an earlier-filed patent.
The term of a U.S. patent that covers an FDA-approved drug may also be eligible for patent term extension, which permits patent term restoration as compensation for the patent term lost during the FDA regulatory review process. The Hatch-Waxman Amendments permit a patent term extension of up to five years beyond the statutory 20 year term of the patent for the approved product. The length of the patent term extension is related to the length of time the drug is under regulatory review. A patent term extension cannot extend the remaining term of a patent beyond a total of 14 years from the date of product approval and only one patent applicable to an approved drug may be extended. Similar provisions are available in Europe and some other foreign jurisdictions to extend the term of a patent that covers an approved drug. When possible, depending upon the length of clinical trials and other factors involved in the filing of a new drug application, or NDA, we expect to apply for patent term extensions for patents covering our product candidates and their methods of use.
The patent portfolios for our proprietary technology platform and our three most advanced product candidates as of March 21, 2014 are summarized below.
TNX-102 SL
Our VLD CBP bedtime treatment technology was discovered by Dr. Iredell W. Iglehart, MD and was sold to Vela Pharmaceuticals and is termed the “Iglehart Technology”. We acquired the Iglehart Technology from L&L, which acquired it from Vela Pharmaceuticals. The patent portfolio for TNX-102 SL relating to the Iglehart Technology includes patent applications directed to pharmaceutical compositions containing CBP, CBP formulations, and methods for treating FM and other CNS conditions utilizing CBP. The Iglehart Technology portfolio includes issued U.S. patents, such as U.S. Patent Nos. 6,541,523, 6,395,788 and 6,358,944, and corresponding issued foreign counterpart patents or applications. U.S. Patent Nos. 6,541,523, 6,395,788 and 6,358,944 are expected to expire in 2020, unless they are eligible for patent term extensions on the basis of FDA approvals.
The unique pharmacokinetic profile of TNX-102 was discovered by Tonix and its development partners and is termed the “PK Technology.” The patent portfolio for TNX-102 SL relating to the PK Technology includes patent applications directed to pharmaceutical compositions containing CBP, CBP formulations, and methods for treating FM and other CNS conditions utilizing CBP. The PK Technology patent portfolio includes U.S. Patent Application No. 13/918,692. If U.S. and non-U.S. patents claiming priority from those applications issue, those patents would expire in 2033, excluding any patent term adjustments or extensions.
Certain Eutectic Compositions were discovered by development partners and are termed the “Eutectic Technology.” The patent portfolio for TNX-102 SL relating to the Eutectic Technology includes patent applications directed to eutectic compositions containing CBP, eutectic CBP formulations, methods for treating FM and other CNS conditions utilizing eutectic CBP compositions, and methods of manufacturing eutectic CBP compositions. The Eutectic Technology patent portfolio includes U.S. patent applications, such as U.S. Patent Application No. 14/214,433. If U.S. and non-U.S. patents claiming priority from those applications issue, those patents would expire in 2034, excluding any patent term adjustments or extensions.
TNX-201 — Isometheptene Isomers
The patent portfolio for TNX-201, relating to isometheptene isomers and termed the “Isometheptene Technology” includes patent applications directed to a purified isomer of isometheptene, pharmaceutical compositions containing isometheptene, isometheptene formulations, methods for modulating headache and other CNS conditions and treating CNS conditions utilizing isometheptene isomers, and methods of manufacturing isometheptene isomers. The Isometheptene Technology patent portfolio includes U.S. Patent Application No. 14/158,735 as well as U.S. Provisional Patent Application Nos. 61/926,739, 61/953,715 and 61/814,664. If U.S. and non-U.S. patents claiming priority from those applications issue, those patents would expire in 2034, excluding any patent term adjustments or extensions.
TNX-301 — Alcoholism Treatment
The patent portfolio for disulfiram and selegiline combinations includes patents and patent applications. It includes claims directed to disulfiram and selegiline, pharmaceutical compositions containing disulfiram and selegiline, disulfiram and selegiline formulations, methods of treating an alcohol use disorder, and methods of modulating alcohol abuse and dependence. It includes issued U.S. Patent Nos. 8,093,300 and 8,481,599. The patent expiring last is expected to expire in 2024, excluding any patent term extensions.
Biodefense Technologies
We are currently developing TNX-102 SL for the management of post-traumatic stress disorder, an indication that is relevant to biodefense. In March 2014, we acquired the rights to develop two additional biodefense technologies: a new drug candidate that potentially protects humans from certain effects of radiation and a new vaccine candidate against smallpox. With respect to the radioprotection drug candidate, we acquired U.S. non-provisional Patent Application No. 14,203,733 and related intellectual property rights. The radio- and chemo-protective technology relates to proprietary forms of a small molecular pharmaceutical agent, which is believed to protect against ionizing radiation after oral administration. With respect to the smallpox vaccine candidate, the Company acquired US non-provisional Patent Application No. 14,207,727 and related intellectual property rights. The smallpox vaccine technology relates to proprietary forms of live vaccinia vaccines which may be safer than ACAM2000, the only currently available replication competent, live vaccinia vaccine to protect against smallpox disease. We believe that these technologies, after further development, may be of interest to biodefense agencies in the U.S. and other countries.
Trade Secrets
In addition to patents, we rely on trade secrets and know-how to develop and maintain our competitive position. For example, significant aspects of our proprietary technology platform are based on unpatented trade secrets and know-how. Trade secrets and know-how can be difficult to protect. We seek to protect our proprietary technology and processes, in part, by confidentiality agreements and invention assignment agreements with our employees, consultants, scientific advisors, contractors, and commercial partners. These agreements are designed to protect our proprietary information and, in the case of the invention assignment agreements, to grant us ownership of technologies that are developed through a relationship with a third party. We also seek to preserve the integrity and confidentiality of our data and trade secrets by maintaining physical security of our premises and physical and electronic security of our information technology systems. While we have confidence in these individuals, organizations and systems, agreements or security measures may be breached, and we may not have adequate remedies for any breach. In addition, our trade secrets may otherwise become known or be independently discovered by competitors. To the extent that our contractors use intellectual property owned by others in their work for us, disputes may arise as to rights in related or resulting inventions and know-how.
Trademarks
We seek trademark protection in the United States and outside of the United States where available and when appropriate. We have applied for a trademark for Tonix Pharmaceuticals in the United States.
Issued Patents
Our current patents owned are as follows:
Very-Low Dose Cyclobenzaprine
|
Patent No.
|
|
Title
|
|
Country / Region
|
|
Expiration
Date
|
|
6,541,523
|
|
Methods for Treating or Preventing Fibromyalgia Using Very Low Doses of Cyclobenzaprine
|
|
U.S.A
|
|
Aug. 11, 2020
|
|
|
|
|
|
|
|
|
|
6,395,788
|
|
Methods and Compositions for Treating or Preventing Sleep Disturbances and Associated Illnesses Using Very Low Doses of Cyclobenzaprine
|
|
U.S.A.
|
|
Aug. 11, 2020
|
|
|
|
|
|
|
|
|
|
6,358,944
|
|
Method and Compositions for Treating Generalized Anxiety Disorder
|
|
U.S.A.
|
|
Aug. 23, 2020
|
|
|
|
|
|
|
|
|
|
299369
|
|
Uses Compositions for Treating or Preventing Sleep Disturbances Using Very Low Doses of Cyclobenzaprine
|
|
Austria
|
|
Aug. 11, 2020
|
|
|
|
|
|
|
|
|
|
1202722
|
|
Uses Compositions for Treating or Preventing Sleep Disturbances Using Very Low Doses of Cyclobenzaprine
|
|
Belgium, France, Ireland, Luxembourg, Monaco, Portugal, Switzerland, U.K.
|
|
Aug. 11, 2020
|
|
|
|
|
|
|
|
|
|
60021266.1
|
|
Uses Compositions for Treating or Preventing Sleep Disturbances Using Very Low Doses of Cyclobenzaprine
|
|
Germany
|
|
Aug. 11, 2020
|
|
|
|
|
|
|
|
|
|
2245944
|
|
Uses Compositions for Treating or Preventing Sleep Disturbances Using Very Low Doses of Cyclobenzaprine
|
|
Spain
|
|
Aug. 11, 2020
|
|
|
|
|
|
|
|
|
|
1047691
|
|
Uses Compositions for Treating or Preventing Sleep Disturbances Using Very Low Doses of Cyclobenzaprine
|
|
Hong Kong
|
|
Aug. 11, 2020
|
|
|
|
|
|
|
|
|
|
516749
|
|
Uses Compositions for Treating or Preventing Sleep Disturbances Using Very Low Doses of Cyclobenzaprine
|
|
New Zealand
|
|
Aug. 11, 2020
|
Alcoholism Treatment
|
Patent No.
|
|
Title
|
|
Country / Region
|
|
Expiration
Date
|
|
8,093,300
|
|
Compositions and Methods for Increasing Compliance with Therapies Using Aldehyde Dehydrogenase Inhibitors and Treating Alcoholism
|
|
U.S.A.
|
|
May 23, 2024
|
|
|
|
|
|
|
|
|
|
8,481,599
|
|
Compositions and Methods for increasing compliance with therapies using aldehyde dehydrogenase inhibitors and treating alcoholism
|
|
U.S.A.
|
|
Nov. 4, 2022
|
|
|
|
|
|
|
|
|
|
2002354017
|
|
Compositions and Methods for Increasing Compliance with Therapies Using Aldehyde Dehydrogenase Inhibitors and Treating Alcoholism
|
|
Australia
|
|
Nov. 4, 2022
|
|
|
|
|
|
|
|
|
|
2463987
|
|
Compositions and Methods for Increasing Compliance with Therapies Using Aldehyde Dehydrogenase Inhibitors and Treating Alcoholism
|
|
Canada
|
|
Nov. 4, 2022
|
|
|
|
|
|
|
|
|
|
1441708
|
|
Compositions and Methods for Increasing Compliance with Therapies Using Aldehyde Dehydrogenase Inhibitors and Treating Alcoholism
|
|
Austria, Belgium, Denmark, France, Germany, Luxembourg, Monaco, Portugal, Switzerland, U.K.
|
|
Nov. 4, 2022
|
|
|
|
|
|
|
|
|
|
532583
|
|
Compositions and Methods for Increasing Compliance with Therapies Using Aldehyde Dehydrogenase Inhibitors and Treating Alcoholism
|
|
New Zealand
|
|
Nov. 4, 2022
|
Pending Patent Applications
Our current pending patent applications are as follows:
Sublingual Cyclobenzaprine/Amitriptyline
|
Application No.
|
|
Title
|
|
Country / Region
|
|
13/918,692
|
|
Compositions and Methods for Transmucosal Absorption
|
|
U.S.A.
|
|
|
|
|
|
|
|
P20130102101
|
|
Compositions and Methods for Transmucosal Absorption
|
|
Argentina
|
|
|
|
|
|
|
|
2013/24661
|
|
Compositions and Methods for Transmucosal Absorption
|
|
Gulf Cooperation Council
|
|
|
|
|
|
|
|
102121267
|
|
Compositions and Methods for Transmucosal Absorption
|
|
Taiwan
|
|
|
|
|
|
|
|
2013-000737
|
|
Compositions and Methods for Transmucosal Absorption
|
|
Venezuela
|
|
|
|
|
|
|
|
PCT/US13/46023
|
|
Compositions and Methods for Transmucosal Absorption
|
|
PCT
|
Sublingual Doxepin/Imipramine
|
Application No.
|
|
Title
|
|
Country / Region
|
|
PCT/US14/29688
|
|
Compositions and Methods for Transmucosal Absorption
|
|
PCT
|
PTSD Treatment
|
Application No.
|
|
Title
|
|
Country / Region
|
|
12/948,828
|
|
Methods and Compositions for Treating Symptoms Associated with Post-Traumatic Stress Disorder Using Cyclobenzaprine
|
|
U.S.A.
|
|
|
|
|
|
|
|
10831895.7
|
|
Methods and Compositions for Treating Symptoms Associated with Post-Traumatic Stress Disorder Using Cyclobenzaprine
|
|
European Patent Office
|
|
|
|
|
|
|
|
13103530.6
|
|
Methods and Compositions for Treating Symptoms Associated with Post-Traumatic Stress Disorder Using Cyclobenzaprine
|
|
Hong Kong
|
Sleep Disorder Treatment
|
Application No.
|
|
Title
|
|
Country / Region
|
|
13/157,270
|
|
Methods and Compositions for Treating Fatigue Associated with Disordered Sleep Using Very Low Dose Cyclobenzaprine
|
|
U.S.A.
|
Depression Treatment
|
Application No.
|
|
Title
|
|
Country / Region
|
|
13/412,571
|
|
Methods and Compositions for Treating Depression Using Cyclobenzaprine
|
|
U.S.A.
|
|
|
|
|
|
|
|
2012225548
|
|
Methods and Compositions for Treating Depression Using Cyclobenzaprine
|
|
Australia
|
|
|
|
|
|
|
|
2,829,200
|
|
Methods and Compositions for Treating Depression Using Cyclobenzaprine
|
|
Canada
|
|
|
|
|
|
|
|
12755254.5
|
|
Methods and Compositions for Treating Depression Using Cyclobenzaprine
|
|
European Patent Office
|
|
|
|
|
|
|
|
2013-557811
|
|
Methods and Compositions for Treating Depression Using Cyclobenzaprine
|
|
Japan
|
|
|
|
|
|
|
|
614725
|
|
Methods and Compositions for Treating Depression Using Cyclobenzaprine
|
|
New Zealand
|
Cyclobenzaprine/Amitriptyline Eutectics
|
Application No.
|
|
Title
|
|
Country / Region
|
|
14/214,433
|
|
Eutectic Formulations of Cyclobenzaprine Hydrochloride and Amitriptyline Hydrochloride
|
|
U.S.A.
|
|
|
|
|
|
|
|
PCT/US14/29872
|
|
Eutectic Formulations of Cyclobenzaprine Hydrochloride and Amitriptyline Hydrochloride
|
|
PCT
|
|
|
|
|
|
|
|
Not yet assigned
|
|
Eutectic Formulations of Cyclobenzaprine Hydrochloride and Amitriptyline Hydrochloride
|
|
Taiwan
|
|
|
|
|
|
|
|
Not yet assigned
|
|
Eutectic Formulations of Cyclobenzaprine Hydrochloride and Amitriptyline Hydrochloride
|
|
Venezuela
|
Isometheptene Isomer
|
Application No.
|
|
Title
|
|
Country / Region
|
|
61/814,664
|
|
Isometheptene Isomer
|
|
U.S.A.
|
|
|
|
|
|
|
|
61/926,739
|
|
Isometheptene Isomer Crystals
|
|
U.S.A.
|
|
|
|
|
|
|
|
14/158,735
|
|
Isometheptene Isomer
|
|
U.S.A.
|
|
|
|
|
|
|
|
PCT/US14/12142
|
|
Isometheptene Isomer
|
|
PCT
|
|
|
|
|
|
|
|
61/953,715
|
|
Eutectic Isometheptene Mucate
|
|
U.S.A.
|
Cocaine Addiction Treatment
|
Application No.
|
|
Title
|
|
Country / Region
|
|
13/820,338
|
|
Treatment for Cocaine Addiction
|
|
U.S.A.
|
|
|
|
|
|
|
|
2809966
|
|
Treatment for Cocaine Addiction
|
|
Canada
|
|
|
|
|
|
|
|
2011314358
|
|
Treatment for Cocaine Addiction
|
|
Australia
|
|
|
|
|
|
|
|
11832859.0
|
|
Treatment for Cocaine Addiction
|
|
European Patent Office
|
|
|
|
|
|
|
|
2013-527062
|
|
Treatment for Cocaine Addiction
|
|
Japan
|
|
|
|
|
|
|
|
10-2013-7008187
|
|
Treatment for Cocaine Addiction
|
|
Republic of Korea
|
|
|
|
|
|
|
|
13114135.2
|
|
Treatment for Cocaine Addiction
|
|
Hong Kong
|
Neurocognitive Dysfunction Treatment
|
Application No.
|
|
Title
|
|
Country / Region
|
|
12/151,200
|
|
Method for Treating Neurocognitive Dysfunction
|
|
U.S.A.
|
|
|
|
|
|
|
|
09743321.2
|
|
Method for Treating Neurodegenerative Dysfunction
|
|
European Patent Office
|
|
|
|
|
|
|
|
2723688
|
|
Method for Treating Neurodegenerative Dysfunction
|
|
Canada
|
Novel Smallpox Vaccines
|
Application No.
|
|
Title
|
|
Country / Region
|
|
14207727
|
|
Novel Smallpox Vaccines
|
|
U.S.A.
|
Radio and Chemo Protective Agents
|
Application No.
|
|
Title
|
|
Country / Region
|
|
14203733
|
|
Radio and Chemo Protective Agents
|
|
U.S.A.
|
Trademark Application
We have one trademark application that is pending as follows:
|
Number
|
|
Name
|
|
Jurisdiction
|
|
85088881
|
|
Tonix Pharmaceuticals
|
|
U.S.A.
|
Research and Development
We have one employee dedicated to research and development. We anticipate that our research and development expenditures will increase several fold as we advance TNX-102 SL into late-stage clinical development and advance other candidates in our pipeline. We need to raise additional capital to fund our development plans and there is no certainty that we will be successful in continuing to attract new investments. Our research and development operations are located in New York, NY. We have used, and expect to continue to use, third parties to conduct our preclinical and clinical studies.
Manufacturing
We have contracted with third-party contract manufacturing organizations, or CMOs, for the manufacture of TNX-102 SL for investigational purposes, including preclinical and clinical testing, as follows:
|
CMO
|
|
Purpose
|
|
Lipocine Inc.
|
|
TNX-102 gelcap used in our completed pharmacokinetic study on this candidate
|
|
KABS Laboratories, Inc. (Quebec, Canada)
|
|
TNX-102 intravenous and sublingual solutions
|
|
Laboratorio Farmacologico Milanese S.r.l. (Milan, Italy)
|
|
TNX-102 SL tablets used in our completed pharmacokinetic studies
|
|
Pharmatek Laboratories
|
|
TNX-102 SL tablets being used in our current BESTFIT trial in FM, our current open-label safety extension study, and to be used in our planned POC trial in PTSD
|
|
Patheon
|
|
TNX-102 SL tablet scale-up and packaging development
|
All of our compounds are small molecules, synthesized using industry standard processes, and our drug products are formulated using commercially available raw materials.
Government Regulation
The FDA and other federal, state, local and foreign regulatory agencies impose substantial requirements upon the clinical development, approval, labeling, manufacture, marketing and distribution of drug products. These agencies regulate, among other things, research and development activities and the testing, approval, manufacture, quality control, safety, effectiveness, labeling, storage, record keeping, advertising and promotion of our product candidates. The regulatory approval process is generally lengthy and expensive, with no guarantee of a positive result. Moreover, failure to comply with applicable FDA or other requirements may result in civil or criminal penalties, recall or seizure of products, injunctive relief including partial or total suspension of production, or withdrawal of a product from the market.
The FDA regulates, among other things, the research, manufacture, promotion and distribution of drugs in the United States under the FDCA and other statutes and implementing regulations. The process required by the FDA before prescription drug product candidates may be marketed in the United States generally involves the following:
|
|
· |
completion of extensive nonclinical laboratory tests, animal studies and formulation studies, all performed in accordance with the FDA’s Good Laboratory Practice regulations; |
|
|
· |
submission to the FDA of an IND, which must become effective before human clinical trials may begin; |
|
|
· |
for some products, performance of adequate and well-controlled human clinical trials in accordance with the FDA’s regulations, including Good Clinical Practices, to establish the safety and efficacy of the product candidate for each proposed indication; |
|
|
· |
submission to the FDA of an NDA; |
|
|
· |
satisfactory completion of an FDA preapproval inspection of the manufacturing facilities at which the product is produced to assess compliance with cGMP regulations; and |
|
|
· |
FDA review and approval of the NDA prior to any commercial marketing, sale or shipment of the drug. |
The testing and approval process requires substantial time, effort and financial resources, and we cannot be certain that any approvals for our product candidates will be granted on a timely basis, if at all.
Nonclinical tests include laboratory evaluations of product chemistry, formulation and stability, as well as studies to evaluate toxicity in animals and other animal studies. The results of nonclinical tests, together with manufacturing information and analytical data, are submitted as part of an IND to the FDA. Some nonclinical testing may continue even after an IND is submitted. The IND also includes one or more protocols for the initial clinical trial or trials and an investigator’s brochure. An IND automatically becomes effective 30 days after receipt by the FDA, unless the FDA, within the 30-day time period, raises concerns or questions relating to the proposed clinical trials as outlined in the IND and places the clinical trial on a clinical hold. In such cases, the IND sponsor and the FDA must resolve any outstanding concerns or questions before any clinical trials can begin. Clinical trial holds also may be imposed at any time before or during studies due to safety concerns or non-compliance with regulatory requirements. An independent institutional review board, or IRB, at each of the clinical centers proposing to conduct the clinical trial must review and approve the plan for any clinical trial before it commences at that center. An IRB considers, among other things, whether the risks to individuals participating in the trials are minimized and are reasonable in relation to anticipated benefits. The IRB also approves the consent form signed by the trial participants and must monitor the study until completed.
Clinical Trials
Clinical trials involve the administration of the product candidate to human subjects under the supervision of qualified medical investigators according to approved protocols that detail the objectives of the study, dosing procedures, subject selection and exclusion criteria, and the parameters to be used to monitor participant safety. Each protocol for a U.S. study is submitted to the FDA as part of the IND.
Human clinical trials are typically conducted in three sequential phases, but the phases may overlap, or be combined.
|
|
· |
Phase 1 clinical trials typically involve the initial introduction of the product candidate into healthy human volunteers. In Phase 1 clinical trials, the product candidate is typically tested for safety, dosage tolerance, absorption, metabolism, distribution, excretion and pharmacodynamics. |
|
|
· |
Phase 2 clinical trials are generally conducted in a limited patient population to gather evidence about the efficacy of the product candidate for specific, targeted indications; to determine dosage tolerance and optimal dosage; and to identify possible adverse effects and safety risks. Phase 2 clinical trials, in particular Phase 2b trials, can be undertaken to evaluate clinical efficacy and to test for safety in an expanded patient population at geographically dispersed clinical trial sites. |
|
|
· |
Phase 3 clinical trials are undertaken to evaluate clinical efficacy and to test for safety in an expanded patient population at geographically dispersed clinical trial sites. The size of Phase 3 clinical trials depends upon clinical and statistical considerations for the product candidate and disease, but sometimes can include several thousand patients. Phase 3 clinical trials are intended to establish the overall risk-benefit ratio of the product candidate and provide an adequate basis for product labeling. |
Clinical testing must satisfy extensive FDA regulations. Reports detailing the results of the clinical trials must be submitted at least annually to the FDA and safety reports must be submitted for serious and unexpected adverse events. Success in early stage clinical trials does not assure success in later stage clinical trials. The FDA, an IRB or we may suspend a clinical trial at any time on various grounds, including a finding that the research subjects or patients are being exposed to an unacceptable health risk.
New Drug Applications
Assuming successful completion of the required clinical trials, the results of product development, nonclinical studies and clinical trials are submitted to the FDA as part of an NDA. An NDA also must contain extensive manufacturing information, as well as proposed labeling for the finished product. An NDA applicant must develop information about the chemistry and physical characteristics of the drug and finalize a process for manufacturing the product in accordance with cGMP. The manufacturing process must be capable of consistently producing quality product within specifications approved by the FDA. The manufacturer must develop methods for testing the quality, purity and potency of the final product. In addition, appropriate packaging must be selected and tested and stability studies must be conducted to demonstrate that the product does not undergo unacceptable deterioration over its shelf life. Prior to approval, the FDA will conduct an inspection of the manufacturing facilities to assess compliance with cGMP.
The FDA reviews all NDAs submitted before it accepts them for filing. The FDA may request additional information rather than accept an NDA for filing. In this event, the NDA must be resubmitted with the additional information and is subject to review before the FDA accepts it for filing. After an application is filed, the FDA may refer the NDA to an advisory committee for review, evaluation and recommendation as to whether the application should be approved and under what conditions. The FDA is not bound by the recommendations of an advisory committee, but it considers them carefully when making decisions. The FDA may deny approval of an NDA if the applicable regulatory criteria are not satisfied. Data obtained from clinical trials are not always conclusive and the FDA may interpret data differently than we interpret the same data. The FDA may issue a complete response letter, which may require additional clinical or other data or impose other conditions that must be met in order to secure final approval of the NDA. If a product receives regulatory approval, the approval may be significantly limited to specific diseases and dosages or the indications for use may otherwise be limited, which could restrict the commercial value of the product. In addition, the FDA may require us to conduct Phase 4 testing which involves clinical trials designed to further assess a drug’s safety and effectiveness after NDA approval, and may require surveillance programs to monitor the safety of approved products which have been commercialized. Once issued, the FDA may withdraw product approval if ongoing regulatory requirements are not met or if safety or efficacy questions are raised after the product reaches the market.
Section 505(b) NDAs
There are two types of NDAs: the Section 505(b)(1) NDA, or full NDA, and the Section 505(b)(2) NDA. We intend to file Section 505(b)(2) NDAs for TNX-102 SL for FM and PTSD, and for certain other products, that might, if accepted by the FDA, save time and expense in the development and testing of our product candidates. Although the clinical development of TNX-201 can be accelerated due to existing marketing experience, we expect to file a Section 505(b)(1) NDA for TNX-201 and for certain other products. A full NDA is submitted under Section 505(b)(1) of the FDCA, and must contain full reports of investigations conducted by the applicant to demonstrate the safety and effectiveness of the drug. A Section 505(b)(2) NDA may be submitted for a drug for which one or more of the investigations relied upon by the applicant was not conducted by or for the applicant and for which the applicant has no right of reference from the person by or for whom the investigations were conducted. A Section 505(b)(2) NDA may be submitted based in whole or in part on published literature or on the FDA’s finding of safety and efficacy of one or more previously approved drugs, which are known as reference drugs. Thus, the filing of a Section 505(b)(2) NDA may result in approval of a drug based on fewer clinical or nonclinical studies than would be required under a full NDA. The number and size of studies that need to be conducted by the sponsor depends on the amount and quality of data pertaining to the reference drug that are publicly available, and on the similarity of and differences between the applicant’s drug and the reference drug. In some cases, extensive, time-consuming, and costly clinical and nonclinical studies may still be required for approval of a Section 505(b)(2) NDA.
Our drug approval strategy for our new formulations of approved chemical entities is to submit Section 505(b)(2) NDAs to the FDA. As such, we plan to submit NDAs under Section 505(b)(2) for TNX-102 SL for FM and PTSD. The FDA may not agree that this product candidate is approvable for FM or PTSD as Section 505(b)(2) NDAs. If the FDA determines that Section 505(b)(2) NDAs are not appropriate and that full NDAs are required for TNX-102 SL, the time and financial resources required to obtain FDA approval for TNX-102 SL could substantially and materially increase, and TNX-102 SL might be less likely to be approved. If the FDA requires full NDAs for TNX-102 SL, or requires more extensive testing and development for some other reason, our ability to compete with alternative products that arrive on the market more quickly than our product candidates would be adversely impacted. If CBP-containing products are withdrawn from the market by the FDA for any reason, we may not be able to reference such products to support our anticipated TNX-102 SL 505(b)(2) NDA, and we may be required to follow the requirements of Section 505(b)(1).
Based on our intent to file under Section 505(b)(2) with respect to our lead product candidate, TNX-102 SL for FM and PTSD, we believe it is unlikely the development process for this product candidate will follow the ordinary course of Phase 1, Phase 2 and Phase 3 studies. Our human pharmacokinetic studies of TNX-102 SL represented the first use of sublingual CBP in humans and could therefore be described as “Phase 1.” However, because these studies compared TNX-102 SL to existing approved formulations of CBP and specified the comparable ability to deliver effective levels of CBP to the bloodstream of FM patients, these studies provide a reference to the therapeutic effects previously observed in our dose-ranging clinical study of TNX-102 capsules in FM patients. For these reasons, rather than always identifying clinical trials by Phase, we find it more illustrative to describe in a narrative form the purpose of the studies and the nature and potential significance of the results. Because our double-blind, randomized, placebo-controlled, dose-ranging study on bedtime CBP was performed in Canada, we did not meet with the FDA’s Center for Drug Evaluation and Research to discuss our approach and plans until August 2011. In February 2013, we held an End-of-Phase 2/Pre-Phase 3 meeting with the FDA to discuss the clinical and nonclinical requirements to register TNX-102 SL for the management of FM based on the 505(b)(2) regulatory pathway.
Patent Protections
An applicant submitting a Section 505(b)(2) NDA must certify to the FDA with respect to the patent status of the reference drug upon which the applicant relies in support of approval of its drug. With respect to every patent listed in the FDA’s Orange Book, which is the FDA’s list of approved drug products, as claiming the reference drug or an approved method of use of the reference drug, the Section 505(b)(2) applicant must certify that: (1) there is no patent information listed by the FDA for the reference drug; (2) the listed patent has expired; (3) the listed patent has not expired, but will expire on a particular date; (4) the listed patent is invalid, unenforceable, or will not be infringed by the manufacture, use, or sale of the product in the Section 505(b)(2) NDA; or (5) if the patent is a use patent, that the applicant does not seek approval for a use claimed by the patent. If the applicant files a certification to the effect of clause (1), (2) or (5), FDA approval of the Section 505(b)(2) NDA may be made effective immediately upon successful FDA review of the application, in the absence of marketing exclusivity delays, which are discussed below. If the applicant files a certification to the effect of clause (3), the Section 505(b)(2) NDA approval may not be made effective until the expiration of the relevant patent and the expiration of any marketing exclusivity delays.
If the Section 505(b)(2) NDA applicant provides a certification to the effect of clause (4), referred to as a paragraph IV certification, the applicant also must send notice of the certification to the patent owner and the holder of the NDA for the reference drug. The filing of a patent infringement lawsuit within 45 days of the receipt of the notification may prevent the FDA from approving the Section 505(b)(2) NDA for 30 months from the date of the receipt of the notification unless the court determines that a longer or shorter period is appropriate because either party to the action failed to reasonably cooperate in expediting the action. However, the FDA may approve the Section 505(b)(2) NDA before the 30 months have expired if a court decides that the patent is invalid, unenforceable, or not infringed, or if a court enters a settlement order or consent decree stating the patent is invalid or not infringed.
Notwithstanding the approval of many products by the FDA pursuant to Section 505(b)(2), over the last few years certain brand-name pharmaceutical companies and others have objected to the FDA’s interpretation of Section 505(b)(2). If the FDA’s interpretation of Section 505(b)(2) is successfully challenged in court, the FDA may be required to change its interpretation of Section 505(b)(2) which could delay or even prevent the FDA from approving any Section 505(b)(2) NDA that we submit. The pharmaceutical industry is highly competitive, and it is not uncommon for a manufacturer of an approved product to file a citizen petition with the FDA seeking to delay approval of, or impose additional approval requirements for, pending competing products. If successful, such petitions can significantly delay, or even prevent, the approval of the new product. Moreover, even if the FDA ultimately denies such a petition, the FDA may substantially delay approval while it considers and responds to the petition.
Marketing Exclusivity
Market exclusivity provisions under the FDCA can delay the submission or the approval of Section 505(b)(2) NDAs, thereby delaying a Section 505(b)(2) product from entering the market. The FDCA provides five-year marketing exclusivity to the first applicant to gain approval of an NDA for an NCE, meaning that the FDA has not previously approved any other drug containing the same active moiety. This exclusivity prohibits the submission of a Section 505(b)(2) NDA for any drug product containing the active ingredient during the five-year exclusivity period. However, submission of a Section 505(b)(2) NDA that certifies that a listed patent is invalid, unenforceable, or will not be infringed, as discussed above, is permitted after four years, but if a patent infringement lawsuit is brought within 45 days after such certification, FDA approval of the Section 505(b)(2) NDA may automatically be stayed until 7½ years after the NCE approval date. The FDCA also provides three years of marketing exclusivity for the approval of new and supplemental NDAs for product changes, including, among other things, new indications, dosage forms, routes of administration or strengths of an existing drug, or for a new use, if new clinical investigations, other than bioavailability studies, that were conducted or sponsored by the applicant are deemed by FDA to be essential to the approval of the application. Five-year and three-year exclusivity will not delay the submission or approval of another full NDA; however, as discussed above, an applicant submitting a full NDA under Section 505(b)(1) would be required to conduct or obtain a right of reference to all of the preclinical and adequate and well-controlled clinical trials necessary to demonstrate safety and effectiveness.
Other types of exclusivity in the United States include orphan drug exclusivity and pediatric exclusivity. The FDA may grant orphan drug designation to a drug intended to treat a rare disease or condition, which is generally a disease or condition that affects fewer than 200,000 individuals in the United States, or more than 200,000 individuals in the United States and for which there is no reasonable expectation that the cost of developing and making available in the United States a drug for this type of disease or condition will be recovered from sales in the United States for that drug. Seven-year orphan drug exclusivity is available to a product that has orphan drug designation and that receives the first FDA approval for the indication for which the drug has such designation. Orphan drug exclusivity prevents approval of another application for the same drug for the same orphan indication, for a period of seven years, regardless of whether the application is a full NDA or a Section 505(b)(2) NDA, except in limited circumstances, such as a showing of clinical superiority to the product with orphan exclusivity. Pediatric exclusivity, if granted, provides an additional six months to an existing exclusivity or statutory delay in approval resulting from a patent certification. This six-month exclusivity, which runs from the end of other exclusivity protection or patent delay, may be granted based on the voluntary completion of a pediatric study in accordance with an FDA-issued “Written Request” for such a study.
Section 505(b)(2) NDAs are similar to full NDAs filed under Section 505(b)(1) in that they are entitled to any of these forms of exclusivity if they meet the qualifying criteria. They also are entitled to the patent protections described above, based on patents that are listed in the FDA’s Orange Book in the same manner as patents claiming drugs and uses approved for NDAs submitted as full NDAs.
Breakthrough Therapy Designation
On July 9, 2012, the Food and Drug Administration Safety and Innovation Act, or FDASIA, was signed. FDASIA Section 902 provides for a new drug designation –Breakthrough Therapy. A Breakthrough Therapy is a drug:
|
|
· |
intended alone or in combination with one or more other drugs to treat a serious or life threatening disease or condition; and |
|
|
· |
preliminary clinical evidence indicates that the drug may demonstrate substantial improvement over existing therapies on one or more clinically significant endpoints, such as substantial treatment effects observed early in clinical development. |
If a drug is designated as Breakthrough Therapy, the FDA will expedite the development and review of such drug. In the event that our POC study of TNX-102 SL in PTSD is successful, we will request Breakthrough Therapy designation for TNX-102 SL. The Breakthrough Therapy designation process is relatively new, and the majority of requests for designation have been denied. We cannot predict the likelihood of success in seeking Breakthrough Therapy designation.
Other Regulatory Requirements
Maintaining substantial compliance with appropriate federal, state and local statutes and regulations requires the expenditure of substantial time and financial resources. Drug manufacturers are required to register their establishments with the FDA and certain state agencies, and after approval, the FDA and these state agencies conduct periodic unannounced inspections to ensure continued compliance with ongoing regulatory requirements, including cGMPs. In addition, after approval, some types of changes to the approved product, such as adding new indications, manufacturing changes and additional labeling claims, are subject to further FDA review and approval. The FDA may require post-approval testing and surveillance programs to monitor safety and the effectiveness of approved products that have been commercialized. Any drug products manufactured or distributed by us pursuant to FDA approvals are subject to continuing regulation by the FDA, including:
|
|
· |
record-keeping requirements; |
|
|
· |
reporting of adverse experiences with the drug; |
|
|
· |
providing the FDA with updated safety and efficacy information; |
|
|
· |
reporting on advertisements and promotional labeling; |
|
|
· |
drug sampling and distribution requirements; and |
|
|
· |
complying with electronic record and signature requirements. |
In addition, the FDA strictly regulates labeling, advertising, promotion and other types of information on products that are placed on the market. There are numerous regulations and policies that govern various means for disseminating information to health-care professionals as well as consumers, including to industry sponsored scientific and educational activities, information provided to the media and information provided over the Internet. Drugs may be promoted only for the approved indications and in accordance with the provisions of the approved label.
The FDA has very broad enforcement authority and the failure to comply with applicable regulatory requirements can result in administrative or judicial sanctions being imposed on us or on the manufacturers and distributors of our approved products, including warning letters, refusals of government contracts, clinical holds, civil penalties, injunctions, restitution and disgorgement of profits, recall or seizure of products, total or partial suspension of production or distribution, withdrawal of approvals, refusal to approve pending applications, and criminal prosecution resulting in fines and incarceration. The FDA and other agencies actively enforce the laws and regulations prohibiting the promotion of off-label uses, and a company that is found to have improperly promoted off-label uses may be subject to significant liability. In addition, even after regulatory approval is obtained, later discovery of previously unknown problems with a product may result in restrictions on the product or even complete withdrawal of the product from the market.
Food and Drug Administration Amendments Act of 2007
In September 2007, the Food and Drug Administration Amendments Act of 2007, or FDAAA, became law. This legislation grants significant new powers to the FDA, many of which are aimed at improving drug safety and assuring the safety of drug products after approval. In particular, the new law authorizes the FDA to, among other things, require post-approval studies and clinical trials, mandate changes to drug labeling to reflect new safety information, and require risk evaluation and mitigation strategies for certain drugs, including certain currently approved drugs. In addition, the new law significantly expands the federal government’s clinical trial registry and results databank and creates new restrictions on the advertising and promotion of drug products. Under the FDAAA, companies that violate these and other provisions of the new law are subject to substantial civil monetary penalties.
The FDA has not yet implemented many of the provisions of the FDAAA, so we cannot predict the impact of the new legislation on the pharmaceutical industry or our business. However, the requirements and changes imposed by the FDAAA may make it more difficult, and more costly, to obtain and maintain approval for new pharmaceutical products, or to produce, market and distribute existing products. In addition, the FDA’s regulations, policies and guidance are often revised or reinterpreted by the agency or the courts in ways that may significantly affect our business and our products. It is impossible to predict whether additional legislative changes will be enacted, or FDA regulations, guidance or interpretations changed, or what the impact of such changes, if any, may be.
Employees
As of March 26, 2014, we had six full-time employees, of whom three are executives, one is finance and investor relations, and two are administrative. None of our employees are represented by a labor union, and we believe that our relations with our employees are good.
ITEM 1A - RISK FACTORS
RISKS RELATED TO OUR BUSINESS
We have a history of operating losses and expect to incur losses for the foreseeable future. We may never generate revenues or, if we are able to generate revenues, achieve profitability.
We are focused on product development, and we have not generated any revenues to date. We have incurred losses in each year of our operations, and we expect to continue to incur operating losses for the foreseeable future. These operating losses have adversely affected and are likely to continue to adversely affect our working capital, total assets and shareholders’ equity.
The Company and its prospects should be examined in light of the risks and difficulties frequently encountered by new and early stage companies in new and rapidly evolving markets. These risks include, among other things, the speed at which we can scale up operations, our complete dependence upon development of products that currently have no market acceptance, our ability to establish and expand our brand name, our ability to expand our operations to meet the commercial demand of our clients, our development of and reliance on strategic and customer relationships and our ability to minimize fraud and other security risks.
The process of developing our products requires significant clinical, development and laboratory testing and clinical trials. In addition, commercialization of our product candidates will require that we obtain necessary regulatory approvals and establish sales, marketing and manufacturing capabilities, either through internal hiring or through contractual relationships with others. We expect to incur substantial losses for the foreseeable future as a result of anticipated increases in our research and development costs, including costs associated with conducting preclinical testing and clinical trials, and regulatory compliance activities.
Our ability to generate revenues and achieve profitability will depend on numerous factors, including success in:
|
|
· |
developing and testing product candidates; |
|
|
· receiving regulatory approvals; |
|
|
· commercializing our products; and |
|
|
· establishing a favorable competitive position. |
Many of these factors will depend on circumstances beyond our control. We cannot assure you that we will ever have a product approved by the FDA, that we will bring any product to market or, if we are successful in doing so, that we will ever become profitable.
We expect to incur substantial additional operating expenses over the next several years as our research, development, pre-clinical testing, and clinical trial activities increase. The amount of future losses and when, if ever, we will achieve profitability are uncertain. We have no products that have generated any commercial revenue, do not expect to generate revenues from the commercial sale of products in the near future, and might never generate revenues from the sale of products. Our ability to generate revenue and achieve profitability will depend on, among other things, successful completion of the development of our product candidates; obtaining necessary regulatory approvals from the FDA; establishing manufacturing, sales, and marketing arrangements with third parties; and raising sufficient funds to finance our activities. We might not succeed at any of these undertakings. If we are unsuccessful at some or all of these undertakings, our business, prospects, and results of operations may be materially adversely affected.
We have a limited operating history and we expect a number of factors to cause our operating results to fluctuate on a quarterly and annual basis, which may make it difficult to predict our future performance.
We are a development stage biopharmaceutical company with a limited operating history. Our operations to date have been primarily limited to developing our technology and undertaking preclinical studies and clinical trials of our lead product candidate, TNX-102 SL. We have not yet obtained regulatory approvals for TNX-102 SL or any of our other product candidates. Consequently, any predictions made about our future success or viability may not be as accurate as they could be if we had a longer operating history or commercialized products. Our financial condition has varied significantly in the past and will continue to fluctuate from quarter-to-quarter or year-to-year due to a variety of factors, many of which are beyond our control. Factors relating to our business that may contribute to these fluctuations include other factors described elsewhere in this annual report and also include:
|
|
· |
our ability to obtain additional funding to develop our product candidates; |
|
|
· |
delays in the commencement, enrollment and timing of clinical trials; |
|
|
· |
the success of our clinical trials through all phases of clinical development, including our trials of TNX-102 SL; |
|
|
· |
any delays in regulatory review and approval of product candidates in clinical development; |
|
|
· |
our ability to obtain and maintain regulatory approval for TNX-102 SL or any of our other product candidates in the United States and foreign jurisdictions; |
|
|
· |
potential side effects of our product candidates that could delay or prevent commercialization, limit the indications for any approved drug, require the establishment of risk evaluation and mitigation strategies, or cause an approved drug to be taken off the market; |
|
|
· |
our dependence on CMOs to supply or manufacture our products; |
|
|
· |
our dependence on CROs to conduct our clinical trials and non-clinical research; |
|
|
· |
our ability to establish or maintain collaborations, licensing or other arrangements; |
|
|
· |
market acceptance of our product candidates; |
|
|
· |
our ability to establish and maintain an effective sales and marketing infrastructure, either through the creation of a commercial infrastructure or through strategic collaborations; |
|
|
· |
competition from existing products or new products that may emerge; |
|
|
· |
the ability of patients or healthcare providers to obtain coverage of or sufficient reimbursement for our products; |
|
|
· |
our ability to leverage our proprietary technology platform to discover and develop additional product candidates; |
|
|
· |
our ability and our licensors’ abilities to successfully obtain, maintain, defend and enforce intellectual property rights important to our business; |
|
|
· |
our ability to attract and retain key personnel to manage our business effectively; |
|
|
· |
our ability to build our finance infrastructure and improve our accounting systems and controls; |
|
|
· |
potential product liability claims; |
|
|
· |
potential liabilities associated with hazardous materials; and |
|
|
· |
our ability to obtain and maintain adequate insurance policies. |
Accordingly, the results of any quarterly or annual periods should not be relied upon as indications of future operating performance.
We have no approved products on the market and therefore do not expect to generate any revenues from product sales in the foreseeable future, if at all.
To date, we have no approved product on the market and have generated no product revenues. We have funded our operations primarily from sales of our securities. We have not received, and do not expect to receive for at least the next several years, if at all, any revenues from the commercialization of our product candidates. To obtain revenues from sales of our product candidates, we must succeed, either alone or with third parties, in developing, obtaining regulatory approval for, manufacturing and marketing drugs with commercial potential. We may never succeed in these activities, and we may not generate sufficient revenues to continue our business operations or achieve profitability.
We are largely dependent on the success of our lead product candidate, TNX-102 SL, and we cannot be certain that this product candidate will receive regulatory approval or be successfully commercialized.
We currently have no products for sale, and we cannot guarantee that we will ever have any drug products approved for sale. We and our product candidates are subject to extensive regulation by the FDA and comparable regulatory authorities in other countries governing, among other things, research, testing, clinical trials, manufacturing, labeling, promotion, selling, adverse event reporting and recordkeeping. We are not permitted to market any of our product candidates in the United States until we receive approval of an NDA for a product candidate from the FDA or the equivalent approval from a foreign regulatory authority. Obtaining FDA approval is a lengthy, expensive and uncertain process. We currently have one lead product candidate, TNX-102 SL for the treatment of FM, and the success of our business currently depends on its successful development, approval and commercialization. Any projected sales or future revenue predictions are predicated upon FDA approval and market acceptance of TNX-102 SL. If projected sales do not materialize for any reason, it would have a material adverse effect on our business and our ability to continue operations.
TNX-102 SL has not completed the clinical development process; therefore, we have not yet submitted an NDA or foreign equivalent or received marketing approval for this product candidate anywhere in the world. The clinical development program for TNX-102 SL may not lead to commercial products for a number of reasons, including if we fail to obtain necessary approvals from the FDA or foreign regulatory authorities because our clinical trials fail to demonstrate to their satisfaction that this product candidate is safe and effective or the clinical program may be put on hold due to unexpected safety issues with marketed CBP products. We may also fail to obtain the necessary approvals if we have inadequate financial or other resources to advance our product candidates through the clinical trial process. Any failure or delay in completing clinical trials or obtaining regulatory approval for TNX-102 SL in a timely manner would have a material adverse impact on our business and our stock price.
We may use our financial and human resources to pursue a particular research program or product candidate and fail to capitalize on programs or product candidates that may be more profitable or for which there is a greater likelihood of success.
Because we have limited financial and human resources, we are currently focusing on the regulatory approval of TNX-102 SL. As a result, we may forego or delay pursuit of opportunities with other product candidates or for other indications that later prove to have greater commercial potential. Our resource allocation decisions may cause us to fail to capitalize on viable commercial products or profitable market opportunities. Our spending on existing and future product candidates for specific indications may not yield any commercially viable products. If we do not accurately evaluate the commercial potential or target market for a particular product candidate, we may relinquish valuable rights to that product candidate through strategic alliance, licensing or other royalty arrangements in cases in which it would have been more advantageous for us to retain sole development and commercialization rights to such product candidate, or we may allocate internal resources to a product candidate in a therapeutic area in which it would have been more advantageous to enter into a partnering arrangement.
We may need additional capital. If additional capital is not available or is available at unattractive terms, we may be forced to delay, reduce the scope of or eliminate our research and development programs, reduce our commercialization efforts or curtail our operations.
In order to develop and bring our product candidates to market, we must commit substantial resources to costly and time-consuming research, preclinical and clinical trials and marketing activities. We anticipate that our existing cash and cash equivalents will enable us to maintain our current operations for at least the next twelve months. We anticipate using our cash and cash equivalents to fund further research and development with respect to our lead product candidates. We may, however, need to raise additional funding sooner if our business or operations change in a manner that consumes available resources more rapidly than we anticipate. Our requirements for additional capital will depend on many factors, including:
|
|
· |
successful commercialization of our product candidates; |
|
|
· the time and costs involved in obtaining regulatory approval for our product candidates; |
|
|
· costs associated with protecting our intellectual property rights; |
|
|
· development of marketing and sales capabilities; |
|
|
· payments received under future collaborative agreements, if any; and |
|
|
· market acceptance of our products. |
To the extent we raise additional capital through the sale of equity securities, the issuance of those securities could result in dilution to our shareholders. In addition, if we obtain debt financing, a substantial portion of our operating cash flow may be dedicated to the payment of principal and interest on such indebtedness, thus limiting funds available for our business activities. If adequate funds are not available, we may be required to delay, reduce the scope of or eliminate our research and development programs, reduce our commercialization efforts or curtail our operations. In addition, we may be required to obtain funds through arrangements with collaborative partners or others that may require us to relinquish rights to technologies, product candidates or products that we would otherwise seek to develop or commercialize ourselves or license rights to technologies, product candidates or products on terms that are less favorable to us than might otherwise be available.
We will require substantial additional funds to support our research and development activities, and the anticipated costs of preclinical studies and clinical trials, regulatory approvals and eventual commercialization. Such additional sources of financing may not be available on favorable terms, if at all. If we do not succeed in raising additional funds on acceptable terms, we may be unable to initiate clinical trials or obtain approval of any product candidates from the FDA and other regulatory authorities. In addition, we could be forced to discontinue product development, forego sales and marketing efforts and forego attractive business opportunities. Any additional sources of financing will likely involve the issuance of our equity securities, which will have a dilutive effect on our shareholders.
There is no assurance that we will be successful in raising the additional funds needed to fund our business plan. If we are not able to raise sufficient capital in the near future, our continued operations will be in jeopardy and we may be forced to cease operations and sell or otherwise transfer all or substantially all of our remaining assets.
We face intense competition in the markets targeted by our lead product candidates. Many of our competitors have substantially greater resources than we do, and we expect that all of our product candidates under development will face intense competition from existing or future drugs.
We expect that all of our product candidates under development, if approved, will face intense competition from existing and future drugs marketed by large companies. These competitors may successfully market products that compete with our products, successfully identify drug candidates or develop products earlier than we do, or develop products that are more effective, have fewer side effects or cost less than our products.
Additionally, if a competitor receives FDA approval before we do for a drug that is similar to one of our product candidates, FDA approval for our product candidate may be precluded or delayed due to periods of non-patent exclusivity and/or the listing with the FDA by the competitor of patents covering its newly-approved drug product. Periods of non-patent exclusivity for new versions of existing drugs such as our current product candidates can extend up to three and one-half years.
These competitive factors could require us to conduct substantial new research and development activities to establish new product targets, which would be costly and time consuming. These activities would adversely affect our ability to commercialize products and achieve revenue and profits.
Competition and technological change may make our product candidates and technologies less attractive or obsolete.
We compete with established pharmaceutical and biotechnology companies that are pursuing other forms of treatment for the same indications we are pursuing and that have greater financial and other resources. Other companies may succeed in developing products earlier than us, obtaining FDA approval for products more rapidly, or developing products that are more effective than our product candidates. Research and development by others may render our technology or product candidates obsolete or noncompetitive, or result in treatments or cures superior to any therapy we develop. We face competition from companies that internally develop competing technology or acquire competing technology from universities and other research institutions. As these companies develop their technologies, they may develop competitive positions that may prevent, make futile, or limit our product commercialization efforts, which would result in a decrease in the revenue we would be able to derive from the sale of any products.
There can be no assurance that any of our product candidates will be accepted by the marketplace as readily as these or other competing treatments. Furthermore, if our competitors' products are approved before ours, it could be more difficult for us to obtain approval from the FDA. Even if our products are successfully developed and approved for use by all governing regulatory bodies, there can be no assurance that physicians and patients will accept our product(s) as a treatment of choice.
Furthermore, the pharmaceutical research industry is diverse, complex, and rapidly changing. By its nature, the business risks associated therewith are numerous and significant. The effects of competition, intellectual property disputes, market acceptance, and FDA regulations preclude us from forecasting revenues or income with certainty or even confidence.
If we fail to protect our intellectual property rights, our ability to pursue the development of our technologies and products would be negatively affected.
Our success will depend in part on our ability to obtain patents and maintain adequate protection of our technologies and products. If we do not adequately protect our intellectual property, competitors may be able to use our technologies to produce and market drugs in direct competition with us and erode our competitive advantage. Some foreign countries lack rules and methods for defending intellectual property rights and do not protect proprietary rights to the same extent as the United States. Many companies have had difficulty protecting their proprietary rights in these foreign countries. We may not be able to prevent misappropriation of our proprietary rights.
We have received, and are currently seeking, patent protection for numerous compounds and methods of treating diseases. However, the patent process is subject to numerous risks and uncertainties, and there can be no assurance that we will be successful in protecting our products by obtaining and defending patents. These risks and uncertainties include the following: patents that may be issued or licensed may be challenged, invalidated, or circumvented, or otherwise may not provide any competitive advantage; our competitors, many of which have substantially greater resources than us and many of which have made significant investments in competing technologies, may seek, or may already have obtained, patents that will limit, interfere with, or eliminate our ability to make, use, and sell our potential products either in the United States or in international markets; there may be significant pressure on the United States government and other international governmental bodies to limit the scope of patent protection both inside and outside the United States for treatments that prove successful as a matter of public policy regarding worldwide health concerns; countries other than the United States may have less restrictive patent laws than those upheld by United States courts, allowing foreign competitors the ability to exploit these laws to create, develop, and market competing products.
Moreover, any patents issued to us may not provide us with meaningful protection, or others may challenge, circumvent or narrow our patents. Third parties may also independently develop products similar to our products, duplicate our unpatented products or design around any patents on products we develop. Additionally, extensive time is required for development, testing and regulatory review of a potential product. While extensions of patent term due to regulatory delays may be available, it is possible that, before any of our product candidates can be commercialized, any related patent, even with an extension, may expire or remain in force for only a short period following commercialization, thereby reducing any advantages of the patent.
In addition, the United States Patent and Trademark Office (the "PTO") and patent offices in other jurisdictions have often required that patent applications concerning pharmaceutical and/or biotechnology-related inventions be limited or narrowed substantially to cover only the specific innovations exemplified in the patent application, thereby limiting the scope of protection against competitive challenges. Thus, even if we or our licensors are able to obtain patents, the patents may be substantially narrower than anticipated.
Our success depends on our patents, patent applications that may be licensed exclusively to us and other patents to which we may obtain assignment or licenses. We may not be aware, however, of all patents, published applications or published literature that may affect our business either by blocking our ability to commercialize our product candidates, by preventing the patentability of our product candidates to us or our licensors, or by covering the same or similar technologies that may invalidate our patents, limit the scope of our future patent claims or adversely affect our ability to market our product candidates.
In addition to patents, we rely on a combination of trade secrets, confidentiality, nondisclosure and other contractual provisions, and security measures to protect our confidential and proprietary information. These measures may not adequately protect our trade secrets or other proprietary information. If they do not adequately protect our rights, third parties could use our technology, and we could lose any competitive advantage we may have. In addition, others may independently develop similar proprietary information or techniques or otherwise gain access to our trade secrets, which could impair any competitive advantage we may have.
Patent protection and other intellectual property protection is crucial to the success of our business and prospects, and there is a substantial risk that such protections will prove inadequate.
We may be involved in lawsuits to protect or enforce our patents, which could be expensive and time consuming.
The pharmaceutical industry has been characterized by extensive litigation regarding patents and other intellectual property rights, and companies have employed intellectual property litigation to gain a competitive advantage. We may become subject to infringement claims or litigation arising out of patents and pending applications of our competitors, or additional interference proceedings declared by the PTO to determine the priority of inventions. The defense and prosecution of intellectual property suits, PTO proceedings, and related legal and administrative proceedings are costly and time-consuming to pursue, and their outcome is uncertain. Litigation may be necessary to enforce our issued patents, to protect our trade secrets and know-how, or to determine the enforceability, scope, and validity of the proprietary rights of others. An adverse determination in litigation or interference proceedings to which we may become a party could subject us to significant liabilities, require us to obtain licenses from third parties, or restrict or prevent us from selling our products in certain markets. Although patent and intellectual property disputes might be settled through licensing or similar arrangements, the costs associated with such arrangements may be substantial and could include our paying large fixed payments and ongoing royalties. Furthermore, the necessary licenses may not be available on satisfactory terms or at all.
Competitors may infringe our patents, and we may file infringement claims to counter infringement or unauthorized use. This can be expensive, particularly for a company of our size, and time-consuming. In addition, in an infringement proceeding, a court may decide that a patent of ours is not valid or is unenforceable, or may refuse to stop the other party from using the technology at issue on the grounds that our patents do not cover its technology. An adverse determination of any litigation or defense proceedings could put one or more of our patents at risk of being invalidated or interpreted narrowly.
Also, a third party may assert that our patents are invalid and/or unenforceable. There are no unresolved communications, allegations, complaints or threats of litigation related to the possibility that our patents are invalid or unenforceable. Any litigation or claims against us, whether or not merited, may result in substantial costs, place a significant strain on our financial resources, divert the attention of management and harm our reputation. An adverse decision in litigation could result in inadequate protection for our product candidates and/or reduce the value of any license agreements we have with third parties.
Interference proceedings brought before the U.S. Patent and Trademark Office may be necessary to determine priority of invention with respect to our patents or patent applications. During an interference proceeding, it may be determined that we do not have priority of invention for one or more aspects in our patents or patent applications and could result in the invalidation in part or whole of a patent or could put a patent application at risk of not issuing. Even if successful, an interference proceeding may result in substantial costs and distraction to our management.
Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation or interference proceedings, there is a risk that some of our confidential information could be compromised by disclosure. In addition, there could be public announcements of the results of hearings, motions or other interim proceedings or developments. If investors perceive these results to be negative, the price of our common stock could be adversely affected.
If we infringe the rights of third parties we could be prevented from selling products, forced to pay damages, and defend against litigation.
If our products, methods, processes and other technologies infringe the proprietary rights of other parties, we could incur substantial costs and we may have to: obtain licenses, which may not be available on commercially reasonable terms, if at all; abandon an infringing product candidate; redesign our products or processes to avoid infringement; stop using the subject matter claimed in the patents held by others; pay damages; and/or defend litigation or administrative proceedings which may be costly whether we win or lose, and which could result in a substantial diversion of our financial and management resources.
If preclinical testing or clinical trials for our product candidates are unsuccessful or delayed, we will be unable to meet our anticipated development and commercialization timelines.
We rely and expect to continue to rely on third parties, including CROs and outside consultants, to conduct, supervise or monitor some or all aspects of preclinical testing or clinical trials involving our product candidates. We have less control over the timing and other aspects of these preclinical testing or clinical trials than if we performed the monitoring and supervision entirely on our own. Third parties may not perform their responsibilities for our preclinical testing or clinical trials on our anticipated schedule or, for clinical trials, consistent with a clinical trial protocol. Delays in preclinical and clinical testing could significantly increase our product development costs and delay product commercialization. In addition, many of the factors that may cause, or lead to, a delay in the clinical trials may also ultimately lead to denial of regulatory approval of a product candidate.
The commencement of clinical trials can be delayed for a variety of reasons, including delays in:
|
|
· |
demonstrating sufficient safety and efficacy to obtain regulatory approval to commence a clinical trial; |
|
|
· |
reaching agreement on acceptable terms with prospective contract research organizations and trial sites; |
|
|
· |
manufacturing sufficient quantities of a product candidate; and |
|
|
· |
obtaining institutional review board approval to conduct a clinical trial at a prospective site. |
Once a clinical trial has begun, it may be delayed, suspended or terminated by us or the FDA or other regulatory authorities due to a number of factors, including:
|
|
· |
ongoing discussions with the FDA or other regulatory authorities regarding the scope or design of our clinical trials; |
|
|
· |
failure to conduct clinical trials in accordance with regulatory requirements; |
|
|
· |
lower than anticipated recruitment or retention rate of patients in clinical trials; |
|
|
· |
inspection of the clinical trial operations or trial sites by the FDA or other regulatory authorities resulting in the imposition of a clinical hold; |
|
|
· |
lack of adequate funding to continue clinical trials; |
|
|
· |
negative results of clinical trials; or |
If clinical trials are unsuccessful, and we are not able to obtain regulatory approvals for our product candidates under development, we will not be able to commercialize these products, and therefore may not be able to generate sufficient revenues to support our business.
We rely on third parties to conduct, supervise and monitor our clinical trials, and if those third parties perform in an unsatisfactory manner, it may harm our business.
We rely on CROs and clinical trial sites to ensure the proper and timely conduct of our clinical trials. While we have agreements governing their activities, we will have limited influence over their actual performance. We will control only certain aspects of our CROs’ activities. Nevertheless, we will be responsible for ensuring that our clinical trials are conducted in accordance with the applicable protocol, legal, regulatory and scientific standards and our reliance on the CROs does not relieve us of our regulatory responsibilities.
We and our CROs are required to comply with the FDA’s current good clinical practices requirements, or cGCP, for conducting, recording and reporting the results of clinical trials to assure that data and reported results are credible and accurate and that the rights, integrity and confidentiality of clinical trial participants are protected. The FDA enforces these cGCPs through periodic inspections of trial sponsors, principal investigators and clinical trial sites. If we or our CROs fail to comply with applicable cGCPs, the clinical data generated in our clinical trials may be deemed unreliable and the FDA may require us to perform additional clinical trials before approving any marketing applications. Upon inspection, the FDA may determine that our clinical trials did not comply with cGCPs. In addition, our clinical trials, including our Phase 2b/3 trial of TNX-102 SL in FM, will require a sufficiently large number of test subjects to evaluate the safety and effectiveness of a product candidate. Accordingly, if our CROs fail to comply with these regulations or fail to recruit a sufficient number of patients, our clinical trials may be delayed or we may be required to repeat such clinical trials, which would delay the regulatory approval process.
Our CROs are not our employees, and we are not able to control whether or not they devote sufficient time and resources to our clinical trials. These CROs may also have relationships with other commercial entities, including our competitors, for whom they may also be conducting clinical trials, or other drug development activities which could harm our competitive position. If our CROs do not successfully carry out their contractual duties or obligations, fail to meet expected deadlines, or if the quality or accuracy of the clinical data they obtain is compromised due to the failure to adhere to our clinical protocols or regulatory requirements, or for any other reasons, our clinical trials may be extended, delayed or terminated, and we may not be able to obtain regulatory approval for, or successfully commercialize our product candidates. As a result, our financial results and the commercial prospects for such product candidates would be harmed, our costs could increase, and our ability to generate revenues could be delayed.
We also rely on other third parties to store and distribute drug products for our clinical trials. Any performance failure on the part of our distributors could delay clinical development or marketing approval of our product candidates or commercialization of our products, if approved, producing additional losses and depriving us of potential product revenue.
We have never conducted a pivotal clinical trial or submitted an NDA before, and may be unable to do so for TNX-102 SL and other product candidates we are developing.
If our Phase 2b/3 study of TNX-102 SL is successful, we then expect to conduct a Phase 3 confirmatory study in support of product registration. As these trials are intended to provide evidence to support marketing approval by the FDA, they are considered pivotal trials. The conduct of pivotal clinical trials and the submission of a successful NDA is a complicated process. Although members of our management team have extensive industry experience, including in the development, clinical testing and commercialization of drug candidates, our company has never conducted a pivotal clinical trial before, has limited experience in preparing, submitting and prosecuting regulatory filings, and has not submitted an NDA before. Consequently, we may be unable to successfully and efficiently execute and complete these planned clinical trials in a way that leads to NDA submission and approval of TNX-102 SL and other product candidates we are developing. We may require more time and incur greater costs than our competitors and may not succeed in obtaining regulatory approvals of product candidates that we develop. Failure to commence or complete, or delays in, our planned clinical trials would prevent or delay commercialization of TNX-102 SL and other product candidates we are developing.
Our product candidates may cause serious adverse events or undesirable side effects which may delay or prevent marketing approval, or, if approval is received, require them to be taken off the market, require them to include safety warnings or otherwise limit their sales.
Serious adverse events or undesirable side effects from TNX-102 SL or any of our other product candidates could arise either during clinical development or, if approved, after the approved product has been marketed. The results of future clinical trials, including TNX-102 SL, may show that our product candidates cause serious adverse events or undesirable side effects, which could interrupt, delay or halt clinical trials, resulting in delay of, or failure to obtain, marketing approval from the FDA and other regulatory authorities.
If TNX-102 SL or any of our other product candidates cause serious adverse events or undesirable side effects:
|
|
· |
regulatory authorities may impose a clinical hold which could result in substantial delays and adversely impact our ability to continue development of the product; |
|
|
· |
regulatory authorities may require the addition of labeling statements, specific warnings, a contraindication or field alerts to physicians and pharmacies; |
|
|
· |
we may be required to change the way the product is administered, conduct additional clinical trials or change the labeling of the product; |
|
|
· |
we may be required to implement a risk minimization action plan, which could result in substantial cost increases and have a negative impact on our ability to commercialize the product; |
|
|
· |
we may be required to limit the patients who can receive the product; |
|
|
· |
we may be subject to limitations on how we promote the product; |
|
|
· |
sales of the product may decrease significantly; |
|
|
· |
regulatory authorities may require us to take our approved product off the market; |
|
|
· |
we may be subject to litigation or product liability claims; and |
|
|
· |
our reputation may suffer. |
Any of these events could prevent us from achieving or maintaining market acceptance of the affected product or could substantially increase commercialization costs and expenses, which in turn could delay or prevent us from generating significant revenues from the sale of our products.
If we are unable to file for approval under Section 505(b)(2) of the FDCA or if we are required to generate additional data related to safety and efficacy in order to obtain approval under Section 505(b)(2), we may be unable to meet our anticipated development and commercialization timelines.
Our current plans for filing NDAs for our product candidates include efforts to minimize the data we will be required to generate in order to obtain marketing approval for our product candidates and therefore possibly obtain a shortened review period for the applications. We held an End-of-Phase 2/Pre-Phase 3 meeting with the FDA in February 2013 to discuss the development of our lead product candidate, TNX-102 SL, in FM. Although our interactions with the FDA have encouraged our efforts to continue to develop TNX-102 SL for FM, there is no assurance that we will satisfy the FDA’s requirements for approval in this indication. We have not come to any agreement with the FDA as to the nature and extent of studies we may be required to conduct in order to achieve approval of TNX-102 SL in PTSD. The timeline for filing and review of our NDAs is based on our plan to submit those NDAs under Section 505(b)(2) of the FDCA, wherein we will rely in part on data in the public domain or elsewhere. We have not yet filed an NDA under Section 505(b)(2) for any of our lead product candidates. Depending on the data that may be required by the FDA for approval, some of the data may be related to products already approved by the FDA. If the data relied upon is related to products already approved by the FDA and covered by third-party patents we would be required to certify that we do not infringe the listed patents or that such patents are invalid or unenforceable. As a result of the certification, the third-party would have 45 days from notification of our certification to initiate an action against us. In the event that an action is brought in response to such a certification, the approval of our NDA could be subject to a stay of up to 30 months or more while we defend against such a suit. Approval of our product candidates under Section 505(b)(2) may therefore be delayed until patent exclusivity expires or until we successfully challenge the applicability of those patents to our product candidates. Alternatively, we may elect to generate sufficient additional clinical data so that we no longer rely on data which triggers a potential stay of the approval of our product candidates. Even if no exclusivity periods apply to our applications under Section 505(b)(2), the FDA has broad discretion to require us to generate additional data on the safety and efficacy of our product candidates to supplement third-party data on which we may be permitted to rely. In either event, we could be required, before obtaining marketing approval for any of our product candidates, to conduct substantial new research and development activities beyond those we currently plan to engage in order to obtain approval of our product candidates. Such additional new research and development activities would be costly and time consuming.
We may not be able to obtain shortened review of our applications, and the FDA may not agree that our products qualify for marketing approval. If CBP-containing products are withdrawn from the market by the FDA for any reason, we may not be able to reference such products to support a 505(b)(2) NDA for TNX-102 SL, and we may need to fulfill the more extensive requirements of Section 505(b)(1). If we are required to generate additional data to support approval, we may be unable to meet our anticipated development and commercialization timelines, may be unable to generate the additional data at a reasonable cost, or at all, and may be unable to obtain marketing approval of our product candidates.
We will need to expand our operations and increase the size of our company, and we may experience difficulties in managing growth.
As we advance our product candidates through preclinical studies and clinical trials and develop new product candidates, we will need to increase our product development, scientific and administrative headcount to manage these programs. In addition, to meet our obligations as a public company, we will need to increase our general and administrative capabilities. Our management, personnel and systems currently in place may not be adequate to support this future growth. Our need to effectively manage our operations, growth and various projects requires that we:
|
|
· |
successfully attract and recruit new employees with the expertise and experience we will require; |
|
|
· |
manage our clinical programs effectively, which we anticipate being conducted at numerous clinical sites; |
|
|
· |
develop a marketing, distribution and sales infrastructure if we seek to market our products directly; and |
|
|
· |
continue to improve our operational, manufacturing, financial and management controls, reporting systems and procedures. |
If we are unable to successfully manage this growth and increased complexity of operations, our business may be adversely affected.
Our executive officers and other key personnel are critical to our business, and our future success depends on our ability to retain them.
Our success depends to a significant extent upon the continued services of Dr. Seth Lederman, our President and Chief Executive Officer. Dr. Lederman has overseen Tonix Sub since inception and provides leadership for our growth and operations strategy as well as being an inventor on many of our patents. Loss of the services of Dr. Lederman would have a material adverse effect on our growth, revenues, and prospective business. We have key-man insurance on the lives of Dr. Lederman, Dr. Leland Gershell, our Chief Financial Officer, and Dr. Bruce Daugherty, our Chief Scientific Officer. We are also highly dependent on our directors and scientific team. We are not aware of any present intention of any of our key personnel to leave our company or to retire. While we have employment agreements with all our executives, they may terminate their employment at any time upon 30 days notice. The loss of any of our key personnel, or the inability to attract and retain qualified personnel, may significantly delay or prevent the achievement of our research, development or business objectives and could materially adversely affect our business, financial condition and results of operations.
Any employment agreement we enter into will not ensure the retention of the employee who is a party to the agreement. In addition, we have only limited ability to prevent former employees from competing with us. Furthermore, our future success will also depend in part on the continued service of our key scientific and management personnel and our ability to identify, hire, and retain additional personnel. We experience intense competition for qualified personnel and may be unable to attract and retain the personnel necessary for the development of our business. Moreover, our work force is located in the "Pharmaceutical Corridor" that spans New York, New Jersey and Pennsylvania, as well as in the San Francisco Bay Area, where competition for personnel with the scientific and technical skills that we seek is extremely high and is likely to remain high. Because of this competition, our compensation costs may increase significantly.
If we are unable to hire additional qualified personnel, our ability to grow our business may be harmed.
Over time we will need to hire additional qualified personnel with expertise in drug development, product registration, clinical and non-clinical research, quality compliance, government regulation, formulation and manufacturing, financial matters and sales and marketing. We compete for qualified individuals with numerous biopharmaceutical companies, universities and other research institutions. Competition for such individuals is intense, and we cannot be certain that our search for such personnel will be successful. Attracting and retaining qualified personnel will be critical to our success.
We rely on third parties to manufacture the compounds used in our trials, and we intend to rely on them for the manufacture of any approved products for commercial sale. If these third parties do not manufacture our product candidates in sufficient quantities and at an acceptable cost, clinical development and commercialization of our product candidates could be delayed, prevented or impaired.
We have no manufacturing facilities, and we have no experience in the clinical or commercial-scale manufacture of drugs or in designing drug manufacturing processes. We intend to rely on CMOs to manufacture some or all of our product candidates in clinical trials and our products that reach commercialization. Completion of our clinical trials and commercialization of our product candidates requires the manufacture of a sufficient supply of our product candidates. We have contracted with outside sources to manufacture our development compounds, including TNX-102 SL. If, for any reason, we become unable to rely on our current sources for the manufacture of our product candidates, either for clinical trials or, at some future date, for commercial quantities, then we would need to identify and contract with additional or replacement third-party manufacturers to manufacture compounds for pre-clinical, clinical, and commercial purposes. Although we are in discussions with other manufacturers we have identified as potential alternative CMOs of TNX-102 SL, we may not be successful in negotiating acceptable terms with any of them.
We believe that there are a variety of manufacturers that we may be able to retain to produce these products. However, once we retain a manufacturing source, if our manufacturers do not perform in a satisfactory manner, we may not be able to develop or commercialize potential products as planned. Certain specialized manufacturers are expected to provide us with modified and unmodified pharmaceutical compounds, including finished products, for use in our preclinical and clinical studies. Some of these materials are available from only one supplier or vendor. Any interruption in or termination of service by such sole source suppliers could result in a delay or interruption in manufacturing until we locate an alternative source of supply. Any delay or interruption in manufacturing operations (or failure to locate a suitable replacement for such suppliers) could materially adversely affect our business, prospects, or results of operations. We do not have any short-term or long-term manufacturing agreements with many of these manufacturers. If we fail to contract for manufacturing on acceptable terms or if third-party manufacturers do not perform as we expect, our development programs could be materially adversely affected. This may result in delays in filing for and receiving FDA approval for one or more of our products. Any such delays could cause our prospects to suffer significantly.
Failure by our third-party manufacturers to comply with the regulatory guidelines set forth by the FDA with respect to our product candidates could delay or prevent the completion of clinical trials, the approval of any product candidates or the commercialization of our products.
Such third-party manufacturers must be inspected by FDA for cGMP compliance before they can produce commercial product. We may be in competition with other companies for access to these manufacturers' facilities and may be subject to delays in manufacture if the manufacturers give other clients higher priority than they give to us. If we are unable to secure and maintain third-party manufacturing capacity, the development and sales of our products and our financial performance may be materially affected.
Manufacturers are obligated to operate in accordance with FDA-mandated requirements. A failure of any of our third-party manufacturers to establish and follow cGMP requirements and to document their adherence to such practices may lead to significant delays in the availability of material for clinical trials, may delay or prevent filing or approval of marketing applications for our products, and may cause delays or interruptions in the availability of our products for commercial distribution following FDA approval. This could result in higher costs to us or deprive us of potential product revenues.
Complying with cGMP and non-U.S. regulatory requirements will require that we expend time, money, and effort in production, recordkeeping, and quality control to assure that the product meets applicable specifications and other requirements. We, or our contracted manufacturing facility, must also pass a pre-approval inspection prior to FDA approval. Failure to pass a pre-approval inspection may significantly delay FDA approval of our products. If we fail to comply with these requirements, we would be subject to possible regulatory action and may be limited in the jurisdictions in which we are permitted to sell our products. As a result, our business, financial condition, and results of operations may be materially harmed.
Drug manufacturers are subject to ongoing periodic unannounced inspections by the FDA, the Drug Enforcement Agency and corresponding state and foreign agencies to ensure strict compliance with cGMP requirements and other requirements under Federal drug laws, other government regulations and corresponding foreign standards. If we or our third-party manufacturers fail to comply with applicable regulations, sanctions could be imposed on us, including fines, injunctions, civil penalties, failure by the government to grant marketing approval of drugs, delays, suspension or withdrawal of approvals, seizures or recalls of product, operating restrictions and criminal prosecutions.
Corporate and academic collaborators may take actions to delay, prevent, or undermine the success of our products.
Our operating and financial strategy for the development, clinical testing, manufacture, and commercialization of drug candidates is heavily dependent on our entering into collaborations with corporations, academic institutions, licensors, licensees, and other parties. Our current strategy assumes that we will successfully establish these collaborations, or similar relationships; however, there can be no assurance that we will be successful establishing such collaborations. Some of our existing collaborations are, and future collaborations may be, terminable at the sole discretion of the collaborator. Replacement collaborators might not be available on attractive terms, or at all. The activities of any collaborator will not be within our control and may not be within our power to influence. There can be no assurance that any collaborator will perform its obligations to our satisfaction or at all, that we will derive any revenue or profits from such collaborations, or that any collaborator will not compete with us. If any collaboration is not pursued, we may require substantially greater capital to undertake development and marketing of our proposed products and may not be able to develop and market such products effectively, if at all. In addition, a lack of development and marketing collaborations may lead to significant delays in introducing proposed products into certain markets and/or reduced sales of proposed products in such markets.
Data provided by collaborators and others upon which we rely that has not been independently verified could turn out to be false, misleading, or incomplete.
We rely on third-party vendors, scientists, and collaborators to provide us with significant data and other information related to our projects, clinical trials, and our business. If such third parties provide inaccurate, misleading, or incomplete data, our business, prospects, and results of operations could be materially adversely affected.
Our product candidates are novel and still in development.
We are a pharmaceutical company focused on the development of drug product candidates, all of which are still in development. Our drug development methods may not lead to commercially viable drugs for any of several reasons. For example, we may fail to identify appropriate targets or compounds, our drug candidates may fail to be safe and effective in clinical trials, or we may have inadequate financial or other resources to pursue development efforts for our drug candidates. Our drug candidates will require significant additional development, clinical trials, regulatory clearances and additional investment by us or our collaborators before they can be commercialized.
Successful development of our products is uncertain.
Our development of current and future product candidates is subject to the risks of failure and delay inherent in the development of new pharmaceutical products, including: delays in product development, clinical testing, or manufacturing; unplanned expenditures in product development, clinical testing, or manufacturing; failure to receive regulatory approvals; emergence of superior or equivalent products; inability to manufacture on its own, or through any others, product candidates on a commercial scale; and failure to achieve market acceptance.
Because of these risks, our research and development efforts may not result in any commercially viable products. If a significant portion of these development efforts are not successfully completed, required regulatory approvals are not obtained or any approved products are not commercially successfully, our business, financial condition, and results of operations may be materially harmed.
Clinical trials required for our product candidates are expensive and time-consuming, and their outcome is uncertain.
In order to obtain FDA approval to market a new drug product, we must demonstrate proof of safety and effectiveness in humans. To meet these requirements, we must conduct "adequate and well controlled" clinical trials. Conducting clinical trials is a lengthy, time-consuming, and expensive process. The length of time may vary substantially according to the type, complexity, novelty, and intended use of the product candidate, and often can be several years or more per trial. Delays associated with products for which we are directly conducting clinical trials may cause us to incur additional operating expenses. The commencement and rate of completion of clinical trials may be delayed by many factors, including, for example: inability to manufacture sufficient quantities of qualified materials under cGMP, for use in clinical trials; slower than expected rates of patient recruitment; failure to recruit a sufficient number of patients; modification of clinical trial protocols; changes in regulatory requirements for clinical trials; the lack of effectiveness during clinical trials; the emergence of unforeseen safety issues; delays, suspension, or termination of the clinical trials due to the institutional review board responsible for overseeing the study at a particular study site; and government or regulatory delays or "clinical holds" requiring suspension or termination of the trials.
The results from early clinical trials are not necessarily predictive of results obtained in later clinical trials. Accordingly, even if we obtain positive results from early clinical trials, we may not achieve the same success in future clinical trials. Clinical trials may not demonstrate sufficient safety and effectiveness to obtain the requisite regulatory approvals for product candidates.
Our clinical trials may be conducted in patients with CNS conditions, and in some cases, our products are expected to be used in combination with approved therapies that themselves have significant adverse event profiles. During the course of treatment, these patients could suffer adverse medical events or die for reasons that may or may not be related to our products. We cannot ensure that safety issues will not arise with respect to our products in clinical development.
The failure of clinical trials to demonstrate safety and effectiveness for the desired indications could harm the development of that product candidate and other product candidates. This failure could cause us to abandon a product candidate and could delay development of other product candidates. Any delay in, or termination of, our clinical trials would delay the filing of our NDAs with the FDA and, ultimately, our ability to commercialize our product candidates and generate product revenues. Any change in, or termination of, our clinical trials could materially harm our business, financial condition, and results of operations.
We are subject to extensive and costly government regulation.
Product candidates employing our technology are subject to extensive and rigorous domestic government regulation including regulation by the FDA, the Centers for Medicare and Medicaid Services, other divisions of the United States Department of Health and Human Services, the United States Department of Justice, state and local governments, and their respective foreign equivalents. The FDA regulates the research, development, preclinical and clinical testing, manufacture, safety, effectiveness, record-keeping, reporting, labeling, storage, approval, advertising, promotion, sale, distribution, import, and export of biopharmaceutical products. The FDA regulates small molecule chemical entities as drugs, subject to an NDA under the FDCA. If products employing our technologies are marketed abroad, they will also be subject to extensive regulation by foreign governments, whether or not they have obtained FDA approval for a given product and its uses. Such foreign regulation may be equally or more demanding than corresponding United States regulation.
Government regulation substantially increases the cost and risk of researching, developing, manufacturing, and selling our products. The regulatory review and approval process, which includes preclinical testing and clinical trials of each product candidate, is lengthy, expensive, and uncertain. We or our collaborators must obtain and maintain regulatory authorization to conduct clinical trials. We or our collaborators must obtain regulatory approval for each product we intend to market, and the manufacturing facilities used for the products must be inspected and meet legal requirements. Securing regulatory approval requires the submission of extensive preclinical and clinical data and other supporting information for each proposed therapeutic indication in order to establish the product's safety and efficacy, and in the case of biologics also potency and purity, for each intended use. The development and approval process takes many years, requires substantial resources, and may never lead to the approval of a product.
Even if we are able to obtain regulatory approval for a particular product, the approval may limit the indicated medical uses for the product, may otherwise limit our ability to promote, sell, and distribute the product, may require that we conduct costly post-marketing surveillance, and/or may require that we conduct ongoing post-marketing studies. Material changes to an approved product, such as, for example, manufacturing changes or revised labeling, may require further regulatory review and approval. Once obtained, any approvals may be withdrawn, including, for example, if there is a later discovery of previously unknown problems with the product, such as a previously unknown safety issue.
If we, our collaborators, or our contract manufacturers fail to comply with applicable regulatory requirements at any stage during the regulatory process, such noncompliance could result in, among other things delays in the approval of applications or supplements to approved applications; refusal of a regulatory authority, including the FDA, to review pending market approval applications or supplements to approved applications; warning letters; fines; import and/or export restrictions; product recalls or seizures; injunctions; total or partial suspension of production; civil penalties; withdrawals of previously approved marketing applications or licenses; recommendations by the FDA or other regulatory authorities against governmental contracts; and/or criminal prosecutions.
We do not have, and may never obtain, the regulatory approvals we need to market our product candidates.
Following completion of clinical trials, the results are evaluated and, depending on the outcome, submitted to the FDA in the form of an NDA in order to obtain FDA approval of the product and authorization to commence commercial marketing. In responding to an NDA, the FDA may require additional testing or information, may require that the product labeling be modified, may impose post-approval study or reporting requirements or other restrictions on product distribution, or may deny the application. The FDA has established performance goals for review of NDAs-six months for priority applications and ten months for standard applications. However, the FDA is not required to complete its review within these time periods. The timing of final FDA review and action varies greatly, but can take years in some cases and may involve the input of an FDA advisory committee of outside experts. Product sales in the United States may commence only when an NDA is approved.
To date, we have not applied for or received the regulatory approvals required for the commercial sale of any of our products in the United States or in any foreign jurisdiction. None of our product candidates has been determined to be safe and effective, and we have not submitted an NDA to the FDA or an equivalent application to any foreign regulatory authorities for any of our product candidates.
It is possible that none of our product candidates will be approved for marketing. Failure to obtain regulatory approvals, or delays in obtaining regulatory approvals, may adversely affect the successful commercialization of any drugs or biologics that we or our partners develop, may impose additional costs on us or our collaborators, may diminish any competitive advantages that we or our partners may attain, and/or may adversely affect our receipt of revenues or royalties.
Even if approved, our products will be subject to extensive post-approval regulation.
Once a product is approved, numerous post-approval requirements apply. Among other things, the holder of an approved NDA is subject to periodic and other FDA monitoring and reporting obligations, including obligations to monitor and report adverse events and instances of the failure of a product to meet the specifications in the NDA. Application holders must submit new or supplemental applications and obtain FDA approval for certain changes to the approved product, product labeling, or manufacturing process. Application holders must also submit advertising and other promotional material to the FDA and report on ongoing clinical trials.
Depending on the circumstances, failure to meet these post-approval requirements can result in criminal prosecution, fines, injunctions, recall or seizure of products, total or partial suspension of production, denial or withdrawal of pre-marketing product approvals, or refusal to allow us to enter into supply contracts, including government contracts. In addition, even if we comply with FDA and other requirements, new information regarding the safety or effectiveness of a product could lead the FDA to modify or withdraw product approval.
Even if we obtain regulatory approval to market our product candidates, our product candidates may not be accepted by the market.
Even if the FDA approves one or more of our product candidates, physicians and patients may not accept it or use it. Even if physicians and patients would like to use our products, our products may not gain market acceptance among healthcare payors such as managed care formularies, insurance companies or government programs such as Medicare or Medicaid. Acceptance and use of our products will depend upon a number of factors including: perceptions by members of the health care community, including physicians, about the safety and effectiveness of our drug or device product; cost-effectiveness of our product relative to competing products; availability of reimbursement for our product from government or other healthcare payers; and effectiveness of marketing and distribution efforts by us and our licensees and distributors, if any.
The degree of market acceptance of any pharmaceutical product that we develop will depend on a number of factors, including:
|
|
· |
the safety and effectiveness of our products, including any significant potential side effects (including drowsiness and dry mouth), as compared to alternative products or treatment methods; |
|
|
· |
the timing of market entry as compared to competitive products; |
|
|
· |
flat or declining use of off-label muscle-relaxant products for fibromyalgia prior to the launch of TNX-102 SL; |
|
|
· |
the rate of adoption of our products by doctors and nurses; |
|
|
· |
product labeling or product insert required by the FDA for each of our products; |
|
|
· |
reimbursement policies of government and third-party payors; |
|
|
· |
effectiveness of our sales, marketing and distribution capabilities and the effectiveness of such capabilities of our collaborative partners, if any; and |
|
|
· |
unfavorable publicity concerning our products or any similar products. |
Our product candidates, if successfully developed, will compete with a number of products manufactured and marketed by major pharmaceutical companies, biotechnology companies and manufacturers of generic drugs. Our products may also compete with new products currently under development by others. Physicians, patients, third-party payors and the medical community may not accept and utilize any of our product candidates. If our products do not achieve market acceptance, we will not be able to generate significant revenues or become profitable.
Because we expect sales of our current product candidates, if approved, to generate substantially all of our product revenues for the foreseeable future, the failure of these products to find market acceptance would harm our business and could require us to seek additional financing.
If we fail to establish marketing, sales and distribution capabilities, or fail to enter into arrangements with third parties, we will not be able to create a market for our product candidates.
Our strategy with our lead product candidates is to control, directly or through contracted third parties, all or most aspects of the product development process, including marketing, sales and distribution. Currently, we do not have any sales, marketing or distribution capabilities. In order to generate sales of any product candidates that receive regulatory approval, we must either acquire or develop an internal marketing and sales force with technical expertise and with supporting distribution capabilities or make arrangements with third parties to perform these services for us. The acquisition or development of a sales and distribution infrastructure would require substantial resources, which may divert the attention of our management and key personnel and defer our product development efforts. To the extent that we enter into marketing and sales arrangements with other companies, our revenues will depend on the efforts of others. These efforts may not be successful. If we fail to develop sales, marketing and distribution channels, or enter into arrangements with third parties, we will experience delays in product sales and incur increased costs.
Sales of pharmaceutical products largely depend on the reimbursement of patients' medical expenses by government health care programs and private health insurers. Without the financial support of the government or third-party payors, the market for our products will be limited. These third-party payors are increasingly challenging the price and examining the cost effectiveness of medical products and services. Recent proposals to change the health care system in the United States have included measures that would limit or eliminate payments for medical products and services or subject the pricing of medical treatment products to government control. Significant uncertainty exists as to the reimbursement status of newly approved health care products. Third-party payors may not reimburse sales of our products or enable our collaborators to sell them at profitable prices.
Our business strategy might involve out-licensing product candidates to or collaborating with larger firms with experience in marketing and selling pharmaceutical products. There can be no assurance that we will be able to successfully establish marketing, sales, or distribution relationships; that such relationships, if established, will be successful; or that we will be successful in gaining market acceptance for our products. To the extent that we enter into any marketing, sales, or distribution arrangements with third parties, our product revenues will be lower than if we marketed and sold our products directly, and any revenues we receive will depend upon the efforts of such third-parties. If we are unable to establish such third-party sales and marketing relationships, or choose not to do so, we will have to establish and rely on our own in-house capabilities.
We, as a company, have no experience in marketing or selling pharmaceutical products and currently have no sales, marketing, or distribution infrastructure. To market any of our products directly, we would need to develop a marketing, sales, and distribution force that both has technical expertise and the ability to support a distribution capability. The establishment of a marketing, sales, and distribution capability would significantly increase our costs, possibly requiring substantial additional capital. In addition, there is intense competition for proficient sales and marketing personnel, and we may not be able to attract individuals who have the qualifications necessary to market, sell, and distribute our products. There can be no assurance that we will be able to establish internal marketing, sales, or distribution capabilities. If we are unable to, or choose not to establish these capabilities, or if the capabilities we establish are not sufficient to meet our needs, we will be required to establish collaborative marketing, sales, or distribution relationships with third parties.
In the event that we are successful in bringing any products to market, our revenues may be adversely affected if we fail to obtain acceptable prices or adequate reimbursement for our products from third-party payors.
Our ability to commercialize pharmaceutical products successfully may depend in part on the availability of reimbursement for our products from:
|
|
· |
government and health administration authorities; |
|
|
· private health insurers; and |
|
|
· other third party payors, including Medicare. |
We cannot predict the availability of reimbursement for health care products to be approved in the future. Third-party payors, including Medicare, are challenging the prices charged for medical products and services. Government and other third-party payors increasingly are limiting both coverage and the level of reimbursement for new drugs. Third-party insurance coverage may not be available to patients for any of our products.
The continuing efforts of government and third-party payors to contain or reduce the costs of health care may limit our commercial opportunity. If government and other third-party payors do not provide adequate coverage and reimbursement for any prescription product we bring to market, doctors may not prescribe them or patients may ask to have their physicians prescribe competing drugs with more favorable reimbursement. In some foreign markets, pricing and profitability of prescription pharmaceuticals are subject to government control. In the United States, we expect that there will continue to be federal and state proposals for similar controls. In addition, we expect that increasing emphasis on managed care in the United States will continue to put pressure on the pricing of pharmaceutical products. Cost control initiatives could decrease the price that we receive for any products in the future. Further, cost control initiatives could impair our ability to commercialize our products and our ability to earn revenues from this commercialization.
If we obtain approval to commercialize any approved products outside of the United States, a variety of risks associated with international operations could materially adversely affect our business.
If TNX-102 SL or any of our other product candidates are approved for commercialization outside of the United States, we intend to enter into agreements with third parties to market them on a worldwide basis or in more limited geographical regions. We expect that we will be subject to additional risks related to entering into international business relationships, including:
|
|
· |
different regulatory requirements for drug approvals; |
|
|
· |
reduced protection for intellectual property rights, including trade secret and patent rights; |
|
|
· |
unexpected changes in tariffs, trade barriers and regulatory requirements; |
|
|
· |
economic weakness, including inflation, or political instability in particular foreign economies and markets; |
|
|
· |
compliance with tax, employment, immigration and labor laws for employees living or traveling abroad; |
|
|
· |
foreign taxes, including withholding of payroll taxes; |
|
|
· |
foreign currency fluctuations, which could result in increased operating expenses and reduced revenues, and other obligations incident to doing business in another country; |
|
|
· |
workforce uncertainty in countries where labor unrest is more common than in the United States; |
|
|
· |
production shortages resulting from any events affecting raw material supply or manufacturing capabilities abroad; |
|
|
· |
business interruptions resulting from geopolitical actions, including war and terrorism, or natural disasters including earthquakes, hurricanes, floods and fires; and |
|
|
· |
difficulty in importing and exporting clinical trial materials and study samples. |
We face the risk of product liability claims and may not be able to obtain insurance.
Our business exposes us to the risk of product liability claims that are inherent in the development of drugs. If the use of one or more of our or our collaborators' drugs harms people, we may be subject to costly and damaging product liability claims brought against us by clinical trial participants, consumers, health care providers, pharmaceutical companies or others selling our products. Our inability to obtain sufficient product liability insurance at an acceptable cost to protect against potential product liability claims could prevent or inhibit the commercialization of pharmaceutical products we develop, alone or with collaborators. While we currently carry clinical trial insurance and product liability insurance, we cannot predict all of the possible harms or side effects that may result and, therefore, the amount of insurance coverage we hold now or in the future may not be adequate to cover all liabilities we might incur. We intend to expand our insurance coverage to include the sale of commercial products if we obtain marketing approval for our drug candidates in development, but we may be unable to obtain commercially reasonable product liability insurance for any products approved for marketing. If we are unable to obtain insurance at an acceptable cost or otherwise protect against potential product liability claims, we will be exposed to significant liabilities, which may materially and adversely affect our business and financial position. If we are sued for any injury allegedly caused by our or our collaborators' products, our liability could exceed our total assets and our ability to pay the liability. A product liability claim or series of claims brought against us would decrease our cash and could cause our stock price to fall.
We use hazardous chemicals in our business. Potential claims relating to improper handling, storage or disposal of these chemicals could affect us and be time consuming and costly.
Our research and development processes and/or those of our third party contractors may involve the controlled use of hazardous materials and chemicals. These hazardous chemicals are reagents and solvents typically found in a chemistry laboratory. Our operations also produce hazardous waste products. Federal, state and local laws and regulations govern the use, manufacture, storage, handling and disposal of hazardous materials. While we attempt to comply with all environmental laws and regulations, including those relating to the outsourcing of the disposal of all hazardous chemicals and waste products, we cannot eliminate the risk of contamination from or discharge of hazardous materials and any resultant injury. In the event of such an accident, we could be held liable for any resulting damages and any liability could materially adversely affect our business, financial condition and results of operations.
Compliance with environmental laws and regulations may be expensive. Current or future environmental regulations may impair our research, development or production efforts. We might have to pay civil damages in the event of an improper or unauthorized release of, or exposure of individuals to, hazardous materials. We are not insured against these environmental risks.
If we enter into collaborations with third parties, they might also work with hazardous materials in connection with our collaborations. We may agree to indemnify our collaborators in some circumstances against damages and other liabilities arising out of development activities or products produced in connection with these collaborations.
In addition, the federal, state and local laws and regulations governing the use, manufacture, storage, handling and disposal of hazardous or radioactive materials and waste products may require us to incur substantial compliance costs that could materially adversely affect our business, financial condition and results of operations.
Our insurance policies are expensive and protect us only from some business risks, which will leave us exposed to significant uninsured liabilities.
We carry insurance for most categories of risk that our business may encounter, however, we may not have adequate levels of coverage. We currently maintain general liability, clinical trial, key man, property, workers’ compensation, products liability and directors’ and officers’ insurance, along with an umbrella policy, which collectively costs approximately $200,000 per annum. We cannot provide any assurances that we will be able to maintain existing insurance at current or adequate levels of coverage. Any significant uninsured liability may require us to pay substantial amounts, which would adversely affect our cash position and results of operations.
If we retain collaborative partners and our partners do not satisfy their obligations, we will be unable to develop our partnered product candidates.
In the event we enter into any collaborative agreements, we may not have day-to-day control over the activities of our collaborative partners with respect to any of these product candidates. Any collaborative partner may not fulfill its obligations under these agreements. If a collaborative partner fails to fulfill its obligations under an agreement with us, we may be unable to assume the development of the products covered by that agreement or enter into alternative arrangements with a third party. In addition, we may encounter delays in the commercialization of the product candidate that is the subject of the agreement. Accordingly, our ability to receive any revenue from the product candidates covered by these agreements will be dependent on the efforts of our collaborative partner. We could also become involved in disputes with a collaborative partner, which could lead to delays in or termination of our development and commercialization programs and time-consuming and expensive litigation or arbitration. In addition, any such dispute could diminish our collaborators’ commitment to us and reduce the resources they devote to developing and commercializing our products. Conflicts or disputes with our collaborators, and competition from them, could harm our relationships with our other collaborators, restrict our ability to enter future collaboration agreements and delay the research, development or commercialization of our product candidates. If any collaborative partner terminates or breaches its agreement, or otherwise fails to complete its obligations in a timely manner, our chances of successfully developing or commercializing these product candidates would be materially and adversely affected. We may not be able to enter into collaborative agreements with partners on terms favorable to us, or at all. Our inability to enter into collaborative arrangements with collaborative partners, or our failure to maintain such arrangements, would limit the number of product candidates that we could develop and ultimately, decrease our sources of any future revenues.
RISKS RELATED TO OUR STOCK
Sales of additional shares of our common stock, including by us or our directors and officers following expiration or early release of the lock-up periods, could cause the price of our common stock to decline.
Sales of substantial amounts of our common stock in the public market, or the availability of such shares for sale, by us or others, including the issuance of common stock upon exercise of outstanding options and warrants, could adversely affect the price of our common stock. In connection with a public offering in January 2014, our directors and officers have entered into lock-up agreements for 90 days following such offering (which period may be extended under certain circumstances). Our directors and officers may be released from lock-up prior to the expiration of the lock-up periods at the sole discretion of Roth Capital Partners, LLC. We may sell additional shares and our directors and officers, upon expiration or earlier release of the lock-up, may sell shares into the market, which could adversely affect the market price of shares of our common stock.
Our failure to meet the continued listing requirements of The NASDAQ Capital Market could result in a de-listing of our common stock.
If we fail to satisfy the continued listing requirements of The NASDAQ Capital Market, such as the corporate governance requirements or the minimum closing bid price requirement, NASDAQ may take steps to de-list our common stock. Such a de-listing would likely have a negative effect on the price of our common stock and would impair your ability to sell or purchase our common stock when you wish to do so. In the event of a de-listing, we would take actions to restore our compliance with NASDAQ’s listing requirements, but we can provide no assurance that any such action taken by us would allow our common stock to become listed again, stabilize the market price or improve the liquidity of our common stock, prevent our common stock from dropping below the NASDAQ minimum bid price requirement or prevent future non-compliance with NASDAQ’s listing requirements.
The market price for our common stock may be volatile, and your investment in our common stock could decline in value.
The stock market in general has experienced extreme price and volume fluctuations. The market prices of the securities of biotechnology and pharmaceutical companies, particularly companies like ours without product revenues and earnings, have been highly volatile and may continue to be highly volatile in the future. This volatility has often been unrelated to the operating performance of particular companies. The following factors, in addition to other risk factors described in this section, may have a significant impact on the market price of our common stock:
|
|
· |
announcements of technological innovations or new products by us or our competitors; |
|
|
· |
announcement of FDA approval or disapproval of our products or other product-related actions; |
|
|
· |
developments involving our discovery efforts and clinical trials; |
|
|
· |
developments or disputes concerning patents or proprietary rights, including announcements of infringement, interference or other litigation against us or our potential licensees; |
|
|
· |
developments involving our efforts to commercialize our products, including developments impacting the timing of commercialization; |
|
|
· |
announcements concerning our competitors, or the biotechnology, pharmaceutical or drug delivery industry in general; |
|
|
· |
public concerns as to the safety or efficacy of our products or our competitors’ products; |
|
|
· |
changes in government regulation of the pharmaceutical or medical industry; |
|
|
· |
changes in the reimbursement policies of third party insurance companies or government agencies; |
|
|
· |
actual or anticipated fluctuations in our operating results; |
|
|
· |
changes in financial estimates or recommendations by securities analysts; |
|
|
· |
developments involving corporate collaborators, if any; |
|
|
· |
changes in accounting principles; and |
|
|
· |
the loss of any of our key scientific or management personnel. |
In the past, securities class action litigation has often been brought against companies that experience volatility in the market price of their securities. Whether or not meritorious, litigation brought against us could result in substantial costs and a diversion of management’s attention and resources, which could adversely affect our business, operating results and financial condition.
We do not anticipate paying dividends on our common stock and, accordingly, shareholders must rely on stock appreciation for any return on their investment.
We have never declared or paid cash dividends on our common stock and do not expect to do so in the foreseeable future. The declaration of dividends is subject to the discretion of our board of directors and will depend on various factors, including our operating results, financial condition, future prospects and any other factors deemed relevant by our board of directors. You should not rely on an investment in our company if you require dividend income from your investment in our company. The success of your investment will likely depend entirely upon any future appreciation of the market price of our common stock, which is uncertain and unpredictable. There is no guarantee that our common stock will appreciate in value.
We expect that our quarterly results of operations will fluctuate, and this fluctuation could cause our stock price to decline.
Our quarterly operating results are likely to fluctuate in the future. These fluctuations could cause our stock price to decline. The nature of our business involves variable factors, such as the timing of the research, development and regulatory pathways of our product candidates, which could cause our operating results to fluctuate.
Due to the possibility of fluctuations in our revenues and expenses, we believe that quarter-to-quarter comparisons of our operating results are not a good indication of our future performance.
The rights of the holders of common stock may be impaired by the potential issuance of preferred stock.
Our articles of incorporation give our board of directors the right to create new series of preferred stock. As a result, the board of directors may, without stockholder approval, issue preferred stock with voting, dividend, conversion, liquidation or other rights which could adversely affect the voting power and equity interest of the holders of common stock. Preferred stock, which could be issued with the right to more than one vote per share, could be utilized as a method of discouraging, delaying or preventing a change of control. The possible impact on takeover attempts could adversely affect the price of our common stock. Although we have no present intention to issue any shares of preferred stock or to create a series of preferred stock, we may issue such shares in the future.
Efforts to comply with recently enacted changes in securities laws and regulations will increase our costs and require additional management resources, and we still may fail to comply.
As directed by Section 404 of the Sarbanes-Oxley Act of 2002, the SEC adopted rules requiring public companies to include a report of management on their internal controls over financial reporting in their annual reports on Form 10-K. In addition, in the event we are no longer a smaller reporting company, the independent registered public accounting firm auditing our financial statements would be required to attest to the effectiveness of our internal controls over financial reporting. Such attestation requirement by our independent registered public accounting firm would not be applicable to us until the report for the year ended December 31, 2014 at the earliest, if at all. If we are unable to conclude that we have effective internal controls over financial reporting or if our independent registered public accounting firm is required to, but is unable to provide us with a report as to the effectiveness of our internal controls over financial reporting, investors could lose confidence in the reliability of our financial statements, which could result in a decrease in the value of our securities.
Because certain of our stockholders control a significant number of shares of our common stock, they may have effective control over actions requiring stockholder approval.
As of March 24, 2014, our directors, executive officers and principal stockholders, and their respective affiliates, beneficially own approximately 21.2% of our outstanding shares of common stock. As a result, these stockholders, acting together, would have the ability to control the outcome of matters submitted to our stockholders for approval, including the election of directors and any merger, consolidation or sale of all or substantially all of our assets. In addition, these stockholders, acting together, would have the ability to control the management and affairs of our company. Accordingly, this concentration of ownership might harm the market price of our common stock by:
|
|
· delaying, deferring or preventing a change in corporate control; |
|
|
· impeding a merger, consolidation, takeover or other business combination involving us; or |
|
|
· discouraging a potential acquirer from making a tender offer or otherwise attempting to obtain control of us. |
If securities or industry analysts do not publish research or reports about our business, or if they change their recommendations regarding our stock adversely, our stock price and trading volume could decline.
The trading market for our common stock will be influenced by the research and reports that industry or securities analysts publish about us or our business. Our research coverage by industry and financial analysts is currently limited. Even if our analyst coverage increases, if one or more of the analysts who cover us downgrade our stock, our stock price would likely decline. If one or more of these analysts cease coverage of our company or fail to regularly publish reports on us, we could lose visibility in the financial markets, which in turn could cause our stock price or trading volume to decline.
ITEM 1B – UNRESOLVED STAFF COMMENTS
Not required under Regulation S-K for “smaller reporting companies.”
ITEM 2 – PROPERTIES
We maintain our principal office at 509 Madison Avenue, Suite 306, New York, New York 10022. Our telephone number at that office is (212) 980-9155 and our fax number is (212) 923-5700. On February 11, 2014, we entered into a Lease Amendment and Expansion Agreement, whereby we agreed to lease additional premises commencing May 1, 2014 and expiring on April 30, 2019. Including the additional premises, the total square footage of our office space is approximately 4,800. An increase to the original Letter of Credit will be required in the amount of $72,354.24.
The amended base rent is as follows:
|
Lease Year
|
|
Amount Per Annum
|
|
|
2014
|
|
$
|
220,085
|
|
|
2015
|
|
$
|
269,844
|
|
|
2016
|
|
$
|
277,509
|
|
|
2017
|
|
$
|
285,404
|
|
|
2018
|
|
$
|
293,537
|
|
|
2019
|
|
$
|
98,758
|
|
Starting April 1, 2014, we will be renting two offices on a month-to-month basis at 900 E. Hamilton, Suite 100, Campbell, California 95008. The combined monthly rent will be approximately $3,240.
We believe that our existing facilities are suitable and adequate to meet our current business requirements. We maintain websites at www.tonixpharma.com and www.krele.com and the information contained on those websites is not deemed to be a part of this annual report.
ITEM 3 - LEGAL PROCEEDINGS
From time to time, we may become involved in various lawsuits and legal proceedings which arise in the ordinary course of business. However, litigation is subject to inherent uncertainties, and an adverse result in these or other matters may arise from time to time that may harm our business. We are currently not aware of any such legal proceedings or claims that we believe will have, individually or in the aggregate, a material adverse effect on our business, financial condition or operating results.
ITEM 4 – MINE SAFETY DISCLOSURES
Not applicable.
PART II
ITEM 5 - MARKET FOR REGISTRANT’S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES
Price Range of Common Stock
On August 9, 2013, our common stock commenced trading on The NASDAQ Capital Market under the symbol “TNXP.” Prior to August 9, 2013, our common stock was traded on the OTCQB under the symbol “TNXP.” Prior to July 23, 2012, our common stock was quoted on the Over-the-Counter Bulletin Board under the symbol “TNXP.OB.” Prior to February 2012, no public trades occurred in our common stock. The following table sets forth, for the periods indicated, the high and low sales prices per share of our common stock as reported by The NASDAQ Stock Market, the OTCQB or the Over-the-Counter Bulletin Board, as applicable.
|
|
|
Fiscal Year 2012
|
|
|
|
|
High
|
|
Low
|
|
|
First Quarter
|
|
$
|
41.20
|
|
$
|
40.00
|
|
|
Second Quarter
|
|
$
|
40.00
|
|
$
|
16.60
|
|
|
Third Quarter
|
|
$
|
20.00
|
|
$
|
14.80
|
|
|
Fourth Quarter
|
|
$
|
16.40
|
|
$
|
5.00
|
|
|
|
|
Fiscal Year 2013
|
|
|
|
|
High
|
|
Low
|
|
|
First Quarter
|
|
$
|
14.60
|
|
$
|
4.80
|
|
|
Second Quarter
|
|
$
|
15.00
|
|
$
|
2.25
|
|
|
Third Quarter
|
|
$
|
7.99
|
|
$
|
3.00
|
|
|
Fourth Quarter
|
|
$
|
11.35
|
|
$
|
3.60
|
|
On March 24, 2014, the closing sale price of our common stock, as reported by The NASDAQ Stock Market, was $11.13 per share. On March 24, 2014, there were 230 holders of record of our common stock.
Dividend Policy
We have never paid any cash dividends on our capital stock and do not anticipate paying any cash dividends on our common stock in the foreseeable future. We intend to retain future earnings to fund ongoing operations and future capital requirements of our business. Any future determination to pay cash dividends will be at the discretion of the Board and will be dependent upon our financial condition, results of operations, capital requirements and such other factors as the Board deems relevant.
ITEM 6 – SELECTED FINANCIAL DATA
Not required under Regulation S-K for “smaller reporting companies.”
ITEM 7 - MANAGEMENT'S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS
This Management's Discussion and Analysis of Financial Condition and Results of Operations includes a number of forward-looking statements that reflect Management's current views with respect to future events and financial performance. You can identify these statements by forward-looking words such as “may” “will,” “expect,” “anticipate,” “believe,” “estimate” and “continue,” or similar words. Those statements include statements regarding the intent, belief or current expectations of us and members of its management team as well as the assumptions on which such statements are based. Prospective investors are cautioned that any such forward-looking statements are not guarantees of future performance and involve risk and uncertainties, and that actual results may differ materially from those contemplated by such forward-looking statements.
Readers are urged to carefully review and consider the various disclosures made by us in this report and in our other reports filed with the Securities and Exchange Commission. Important factors known to us could cause actual results to differ materially from those in forward-looking statements. We undertake no obligation to update or revise forward-looking statements to reflect changed assumptions, the occurrence of unanticipated events or changes in the future operating results over time. We believe that its assumptions are based upon reasonable data derived from and known about our business and operations and the business and operations of the Company. No assurances are made that actual results of operations or the results of our future activities will not differ materially from its assumptions. Factors that could cause differences include, but are not limited to, expected market demand for the Company’s services, fluctuations in pricing for materials, and competition.
Business Overview
We are a pharmaceutical company dedicated to the development of novel pharmaceutical products for challenging disorders of the CNS. We have a pipeline of product candidates led by TNX-102 SL, which is in pivotal development for FM and represents a new class of medication for this disorder. We expect to report initial results from our ongoing Phase 2b/3 trial of TNX-102 SL in FM in the fourth quarter of 2014. TNX-102 SL is also in development for PTSD, and is expected to enter a Phase 2 trial in this indication in the third quarter of 2014. We are developing TNX-201 for the treatment of ETTH, and we plan to begin clinical studies of TNX-201 in the fourth quarter of 2014. We hold worldwide commercialization rights to TNX-102 SL and TNX-201. Our pipeline also includes a program for the treatment of alcohol abuse and dependence, and protection from smallpox and radiation exposure.
We are pursuing FM as our lead indication for TNX-102 SL. Our therapeutic strategy is supported by positive results from a Phase 2a trial of TNX-102 capsules in FM patients, which demonstrated a significant decrease in pain and other symptoms after eight weeks of treatment. Following the completion of this study, as well the completion of several clinical pharmacokinetic studies of TNX-102 SL, we met with the FDA and announced that the agency indicated that positive results from two adequate, well-controlled safety and efficacy studies as well as the fulfillment of long-term safety exposure requirements for chronic use would support the approval of TNX-102 SL for the management of FM. We are currently conducting a Phase 2b/3 clinical trial of TNX-102 SL for the improvement of pain in people with FM (the BESTFIT trial), from which we expect to report initial results in the fourth quarter of 2014. We are also conducting a 12-month open-label extension study of TNX-102 SL, into which patients who have completed the BESTFIT study may enroll. Following the completion of the BESTFIT trial, we plan to complete the remaining aspects of our development program that are needed for an NDA submission under Section 505(b)(2), including the conduct at least one more pivotal trial in FM. We believe that TNX-102 SL also has the potential to address a range of other neuropsychiatric conditions, including PTSD. We have met with the FDA to discuss the development of TNX-102 SL for PTSD, and we plan to begin a Phase 2 trial to evaluate its efficacy and safety as a treatment for patients with PTSD in the third quarter of 2014.
We are developing another candidate, TNX-201, for the treatment of ETTH. We have met with the FDA to discuss the development of TNX-201 for ETTH, and we plan to conduct a human pharmacology study in the fourth quarter of 2014. Although the development of TNX-201 will be based on the available information of previously-approved, but currently-unapproved, products that contain the active pharmaceutical ingredient in TNX-201, we believe the marketing approval of TNX-201 will be required to conform with the NDA requirements under Section 505(b)(1).
We also have a pipeline of other product candidates, including TNX-301. We intend to develop TNX-301 under the 505(b)(2) provision as a treatment for alcohol abuse and dependence, and plan to begin formulation work on TNX-301 in 2014.
We also recently acquired rights to intellectual property on two biodefense technologies: one relates to the development of novel smallpox vaccines, and the other the development of protective agents against radiation exposure. We plan to perform non-clinical research and development on these programs in 2014. As we interact with the United States Department of Defense and related biodefense agencies regarding our development of TNX-102 SL for PTSD, we believe these technologies will expand our interaction and cooperation with such agencies. Commercializing certain biodefense products in the United States does not always require human efficacy studies, which leads us to believe the cost and risk of bringing these products to market will be reduced, related to other NCEs or new biologicals.
Recapitalization
On October 7, 2011, we executed and consummated the Share Exchange Agreement with Tonix Sub. Pursuant to the Share Exchange, each share of Tonix Sub’s common stock was exchanged for 0.045 shares of our common stock, and each share of Tonix Sub’s Series A and B preferred stock was exchanged for 0.24 shares of our common stock. Upon completion of the Share Exchange, the Tonix Sub shareholders, including holders of 1,396,982 restricted shares, which were subject to accelerated vesting, received in exchange for all of their shares, an aggregate of 1,133,334 shares of our common stock and our existing shareholders retained 200,000 shares of common stock. The 1,133,334 shares issued to the Tonix Sub shareholders constituted approximately 85% of our 1,333,334 shares of common stock issued and outstanding after the Share Exchange. Upon completion of the Share Exchange, Tonix Sub became our wholly-owned subsidiary. For accounting purposes, the acquisition has been treated as a recapitalization of Tonix Sub, accompanied by the issuance of our common stock for the outstanding common stock of Toxic Sub, which was recorded at a nominal value. The historical financial statements are those of Tonix Sub. The accompanying financial statements give retroactive effect to the recapitalization as if it had occurred on June 7, 2007 (inception date). Also, professional services expenses were allocated to research and development and general and administrative expenses in the cumulative from inception through December 31, 2012 statement of operations to be consistent with the current period’s presentation.
Current Operating Trends
Our current research and development efforts are focused on developing our lead product, TNX-102 SL, but we also expend increasing effort on our other pipeline programs, including TNX-201. Our research and development expenses consist of manufacturing work and the cost of drug ingredients used in such work, fees paid to consultants for work related to clinical trial design and regulatory activities, fees paid to providers for conducting various clinical studies as well as for the analysis of the results of such studies, and for other medical research addressing the potential efficacy and safety of our drugs. We believe that significant investment in product development is a competitive necessity, and we plan to continue these investments in order to be in a position to realize the potential of our product candidates and proprietary technologies.
We are currently conducting our BESTFIT study, a Phase 2b/3 clinical trial of TNX-102 SL in FM. We also plan to begin a Phase 2 trial of TNX-102 SL in PTSD in the third quarter of 2014, as well as advance TNX-201 for ETTH into clinical studies in the fourth quarter of 2014. Clinical trials can be very expensive. If these and additional necessary clinical trials are successful, we plan to prepare and submit applications to the FDA for marketing approval for our drug candidates. This process entails significant costs. As a result of these and other factors, we expect our research and development expenses to increase significantly over the next 12 to 24 months.
We expect that a larger percentage of our research and development expenses in the future will be incurred in support of our current and future preclinical and clinical development programs rather than technology development. These expenditures are subject to numerous uncertainties relating to timing and cost to completion. We test compounds in numerous preclinical studies for safety, toxicology and efficacy. At the appropriate time, subject to the approval of regulatory authorities, we expect to conduct early-stage clinical trials for each drug candidate. We anticipate funding these trials ourselves, and possibly with the assistance of federal grants. As we obtain results from trials, we may elect to discontinue or delay clinical trials for certain products in order to focus our resources on more promising products. Completion of clinical trials may take several years, and the length of time generally varies substantially according to the type, complexity, novelty and intended use of a product candidate.
The commencement and completion of clinical trials for our products may be delayed by many factors, including lack of efficacy during clinical trials, unforeseen safety issues, slower than expected patient recruitment, or government delays. In addition, we may encounter regulatory delays or rejections as a result of many factors, including results that do not support the intended safety or efficacy of our product candidates, perceived defects in the design of clinical trials and changes in regulatory policy during the period of product development. As a result of these risks and uncertainties, we are unable to accurately estimate the specific timing and costs of our clinical development programs or the timing of material cash inflows, if any, from our product candidates. Our business, financial condition and results of operations may be materially adversely affected by any delays in, or termination of, our clinical trials or a determination by the FDA that the results of our trials are inadequate to justify regulatory approval, insofar as cash in-flows from the relevant drug or program would be delayed or would not occur.
Results of Operations
We anticipate that our results of operations will fluctuate for the foreseeable future due to several factors, such as the progress of our research and development efforts and the timing and outcome of regulatory submissions. Due to these uncertainties, accurate predictions of future operations are difficult or impossible to make.
Fiscal year Ended December 31, 2013 Compared to Fiscal year Ended December 31, 2012
Revenues and Cost of Goods Sold. We had no revenues or cost of goods sold during the fiscal years ended December 31, 2013 and 2012.
Research and Development Expenses. Research and development expenses for the fiscal year ended December 31, 2013 were $4,649,782, an increase of $2,066,474, or 80%, from $2,583,308 for the fiscal year ended December 31, 2012. This increase is primarily due to increased development work related to TNX-102 SL, including formulation development, manufacturing, human safety and efficacy as well as pharmacokinetic studies, offset by a decrease in non-clinical studies. In 2013, we incurred $1,161,098, $1,418,589 and $431,871 in manufacturing cost, clinical activities and cost, and non-clinical activities and cost, respectively, as compared to $552,953, $836,278 and $468,509 in 2012, respectively.
General and Administrative Expenses. General and administrative expenses for the fiscal year ended December 31, 2013 were $6,238,661, an increase of $2,160,559, or 53%, from $4,078,102 incurred in the fiscal year ended December 31, 2012. This increase is primarily due to payroll related expenses and professional services.
Payroll related expenses increased to $3,247,689 in the current year from $1,820,877 for the fiscal year ended December 31, 2012, an increase of $1,426,812, or 78%. We incurred $1,717,037 in stock based compensation in connection with the vesting of stock options issued to board members, officers and employees in 2013 as compared to $865,157 in stock based compensation in 2012. The increase in cash payroll related costs of $574,932 was primarily a result of the hiring of new employees as well as employee bonuses.
Professional services for the fiscal year ended December 31, 2013 totaled $1,882,080, an increase of $437,625, or 30%, over the $1,444,455 recognized for the fiscal year ended December 31, 2012. Of professional services, legal fees totaled $902,714 for the fiscal year ended December 31, 2013, an increase of $437,191, or 94%, from $465,523 incurred for the fiscal year ended December 31, 2012. Of the legal fees incurred, $458,143 were patent related costs in the 2013 year as compared to $131,362 in 2012. Consulting fees totaled $735,034 for the fiscal year ended December 31, 2013, an increase of $266 or 0%, from $734,768 for the fiscal year ended December 31, 2012. Accounting fees incurred in the fiscal years ended December 31, 2013 and 2012 amounted to $244,332 and $244,164, respectively.
Travel, meals and entertainment costs for the fiscal year ended December 31, 2013 were $313,883, an increase of $205,635, or 190%, from $108,248 incurred in the fiscal year ended December 31, 2012. Travel, meals and entertainment costs include travel related to investor relations activities, which accounted for the primary increase from 2012. Rent for the fiscal years ended December 31, 2013 and 2012 totaled $116,569 and $116,732, respectively. Market research and analysis for the fiscal year ended December 31, 2013 was $48,161, a decrease of $181,385 or 79% from $229,546 incurred in the fiscal year ended December 31, 2012. Depreciation expense in fiscal 2013 totaled $16,591, an increase of $2,262, or 16%, over the expense of $14,329 incurred in fiscal 2012, as a result of the purchase of new office computers.
Change in fair value of warrant liability. In connection with our January and March 2012 financing, we issued warrants that contained certain reset provisions. As such, we were required to record the fair value as a liability and mark to market each reporting period. In June 2012, upon the effectiveness of our registration statement, these reset provisions expired. Therefore we adjusted the fair value of the warrants from their initial issuance in January and March 2012, charged operations in 2012 for the increase in fair value of $1,177,026 and reclassified the fair value of warrants to equity.
Interest Expense. Interest income for the fiscal year ended December 31, 2013 totaled $4,400, as compared to interest expense of $1,613,043 incurred during the fiscal year ended December 31, 2012, a decrease of $1,617,443. In the fiscal year ended December 31, 2012, our interest costs were comprised primarily of a beneficial conversion feature related to our issuance of convertible debentures in December 2012 charged to interest of $710,000, $196,166 of deferred financing costs related to the issuance of our secured convertible debentures in October 2011 and December 2012, allocated offering costs of $270,743 charged to interest as part of a financing, and the fair value of $426,152, net with prior period accrual, of common stock and warrants issued to convertible debentures holders in connection with the conversion to a financing. In addition, in 2012 we incurred interest expense related to our convertible debentures of $12,292, net with interest income of $2,310.
Net Loss. As a result of the foregoing, net loss for the year ended December 31, 2013 was $10,884,043, compared to a net loss of $9,449,600 for the year ended December 31, 2012.
Liquidity and Capital Resources
As of December 31, 2013, we had working capital of $6,941,189, comprised primarily of cash of $8,201,622, offset by $765,417 of accounts payable, $1,165,670 of accrued expenses and $280,000 of promissory notes to related parties. A significant portion of the accounts payable and accrued expenses are due to work performed in relation to our ongoing Phase 2b/3 clinical trial of TNX-102 SL in FM. For the year ended December 31, 2013 and 2012, we used approximately $8,517,000 and $5,713,000 of cash in operating activities, respectively, which represent cash outlays for research and development and general and administrative expenses in such periods. Increases in cash outlays principally resulted from manufacturing, pre-clinical and clinical cost and activities, regulatory cost, and payroll. For the year ended December 31, 2013, net proceeds from financing activities were from the sale of our common stock and warrants of approximately $10,042,000, the exercise of warrants of $4,581,000, and from the sale of promissory notes to related parties for $280,000. In the comparable 2012 period, approximately $6,933,000 was raised through the sale of shares of common stock and warrants, $320,000 from sale of notes payable and $390,000 from the sale of convertible debentures, net with $150,000 repayments. At December 31, 2013, we had cash of $8,201,622 compared to $1,785,390 at December 31, 2012. Our cash is held in bank deposit accounts.
Cash used in investing activities for the year ended December 31, 2013 was approximately $15,000 reflecting purchase of equipment as compared to cash used for the year ended December 31, 2012 of approximately $36,000 also reflecting purchase of equipment.
August 2013 Public Offering
On August 9, 2013, we entered into an underwriting agreement (the “Underwriting Agreement”) with Roth Capital Partners, LLC, as representative of the underwriters named therein (the “Underwriters”) (the “Underwriters”), pursuant to which we agreed to offer to the public through the Underwriters an aggregate of 2,680,000 units (each a “Unit”, and collectively, the “Units”) at a public offering price of $4.25 per Unit in an underwritten public offering (the "Offering"). Each Unit consists of (i) one share of our common stock and (ii) one Series A Warrant (the “Warrants”) to purchase one share of common stock. Pursuant to the Underwriting Agreement, we also granted the Underwriters an option for a period of 45 days to purchase up to (i) 402,000 additional Units or (ii) 402,000 additional shares of common stock and/or additional Warrants to purchase up to 402,000 shares of common stock, on the same terms, to cover any over-allotments, if any.
The Offering closed on August 14, 2013. The Underwriters purchased the Units at an eight-percent discount to the public offering price, for an aggregate discount of approximately $0.34. We received net cash proceeds of $10,038,013 after deducting underwriting discounts and commissions and offering expenses of $440,787 payable by us associated with the Offering. On August 14, 2013, the Underwriters exercised their over-allotment option to purchase additional Warrants to purchase 402,000 shares of common stock.
The Underwriters also received warrants to purchase up to an aggregate of 107,200 shares of Common Stock, or four percent of the total number of shares included in the Units.
The Warrants are exercisable at an exercise price of $4.25 per share, subject to anti-dilutive adjustment, and expire on the fifth anniversary of the date of issuance. The Warrants will be exercisable on a "cashless" basis in certain circumstances. As of March 26, 2014, 1,184,264 of the Warrants remain outstanding.
The exercise price and number of shares of Common Stock issuable upon exercise of the Warrants will be subject to adjustment in the event of any stock split, reverse stock split, stock dividend, recapitalization, reorganization or similar transaction, as described in the Warrants.
January 2014 Public Offering
On January 24, 2014, we entered into an underwriting agreement (the “Second Underwriting Agreement”) with Roth Capital Partners, LLC, as representative of several underwriters (collectively, the “Second Underwriters”), relating to the issuance and sale of 2,898,550 shares of our common stock. The public offering price for each share of common stock was $15.00.
The net proceeds to the Company from the sale of the shares of common stock was approximately $40.7 million, after deducting underwriting discounts and commissions and other offering expenses payable by the Company. The Company granted the Underwriters a 45-day option to purchase up to an additional 434,782 shares of Common Stock to cover over-allotments, if any. The offering closed on January 29, 2014 and the over-allotment option expired unexercised.
Future Liquidity Requirements
We expect to incur losses from operations for the near future. We expect to incur increasing research and development expenses, including expenses related to additional clinical trials. We expect that our general and administrative expenses will increase in the future as we expand our business development, add infrastructure and incur additional costs related to being a public company, including incremental audit fees, investor relations programs and increased professional services.
Our future capital requirements will depend on a number of factors, including the progress of our research and development of product candidates, the timing and outcome of regulatory approvals, the costs involved in preparing, filing, prosecuting, maintaining, defending and enforcing patent claims and other intellectual property rights, the status of competitive products, the availability of financing and our success in developing markets for our product candidates. We believe our existing cash is sufficient to fund our operating expenses and capital equipment requirements for at least the next 12 months.
We presently do not have any available credit, bank financing or other external sources of liquidity. Due to our history and historical operating losses, our operations have not been a source of liquidity. We may need to obtain additional capital in order to fund future research and development activities. Future financing may include the issuance of equity or debt securities, obtaining credit facilities, or other financing mechanisms. Even if we are able to raise the funds required, it is possible that we could incur unexpected costs and expenses, fail to collect significant amounts owed to us, or experience unexpected cash requirements that would force us to seek alternative financing. Furthermore, if we issue additional equity or debt securities, shareholders may experience additional dilution or the new equity securities may have rights, preferences or privileges senior to those of existing holders of our common stock.
If additional financing is not available or is not available on acceptable terms, we may be required to delay, reduce the scope of or eliminate our research and development programs, reduce our commercialization efforts or obtain funds through arrangements with collaborative partners or others that may require us to relinquish rights to certain product candidates that we might otherwise seek to develop or commercialize independently.
Transactions with Related Parties
We have entered into an agreement with Lederman & Co., LLC (“Lederman & Co”), a company under the control of Dr. Seth Lederman, our Chief Executive Officer and Chairman of the Board of Directors. Effective October 15, 2013, Lederman & Co received $325,000 per annum for its consulting services. On February 11, 2014, the agreement with Lederman & Co was terminated, and the Company simultaneously entered into an employment agreement with Dr. Lederman.
On July 31 and August 1, 2013, we sold three promissory notes in the aggregate principal face amount of $280,000 to two related parties in exchange for $280,000. The notes are payable on demand at any time after one year from issuance and bear no interest.
On March 18, 2014, Tonix Barbados entered into an asset purchase agreement (the “Starling Agreement”) with Starling Pharmaceuticals, Inc. (“Starling”) and an asset purchase agreement (the “Leder Agreement” and together with the Starling Agreement, the “Agreements”) with Leder Laboratories, Inc. (“Leder”). Seth Lederman, the Company’s Chairman and Chief Executive Officer, is the Chairman, CEO and majority owner (through majority-owned entities) of Starling and Leder.
Pursuant to the Starling Agreement, Tonix Barbados acquired from Starling rights to a United States patent application for radio- and chemo-protective agents and related intellectual property rights, in exchange for $125,000 and 25,000 shares of our common stock.
Pursuant to the Leder Agreement, Tonix Barbados acquired from Leder rights to a United States patent application for novel smallpox vaccines and related intellectual property rights, in exchange for $125,000 and 25,000 shares of our common stock.
Stock Compensation
In February 2012, we approved the 2012 Incentive Stock Options Plan, which was amended and restated in February 2013 (“2012 Plan”). The 2012 Plan provides for the issuance of options to purchase up to 550,000 shares of our common stock to officers, directors, employees and consultants. Under the terms of the 2012 Plan, we may issue Incentive Stock Options, as defined by the Internal Revenue Code, and nonstatutory options. The Board of Directors determines the exercise price, vesting and expiration period of the options granted under the 2012 Plan. However, the exercise price of an Incentive Stock Option must be at least 100% of fair value of the common stock at the date of the grant (or 110% for any shareholder that owns 10% or more of our common stock). The fair market value of the common stock determined based on quoted market price or in absence of such quoted market price, by the Board of Directors in a good faith. Additionally, the vesting period of the grants under the 2012 Plan should not be more than five years and expiration period not more than ten years. We reserved 550,000 shares of our common stock for future issuance under the terms of the 2012 Plan.
In May 2012, we issued options to purchase 175,000 shares of common stock pursuant to the 2012 Plan, with such options vesting 1/3rd on May 9, 2013 and 1/36th on the 9th of each month thereafter for 24 months, having an exercise price of $30.00 and expiring 10 years from date of issuance. In February 2013, we issued options to purchase 226,500 shares of common stock pursuant to the 2012 Plan, with such options vesting 1/3rd on February 12, 2014 and 1/36th on the 12th of each month thereafter for 24 months, having an exercise price of $10.20 and expiring 10 years from date of issuance. In February 2014, we issued options to purchase 173,500 shares of common stock pursuant to the 2012 Plan, with such options vesting 1/3rd on February 11, 2015 and 1/36th on the 12th of each month thereafter for 24 months, having an exercise price of $15.88 and expiring 10 years from date of issuance.
Lease Commitments
In September 2010, we entered into a five-year lease for office space in New York City. We issued a letter of credit in the amount of approximately $60,000 for the benefit of the landlord, which is collateralized by a money market account.
On February 11, 2014, we entered into a Lease Amendment and Expansion Agreement, whereby we agreed to lease additional premises commencing May 1, 2014 and expiring on April 30, 2019. Including the additional premises, the total square footage of the office space is approximately 4,776. An increase to the original Letter of Credit will be required in the amount of $72,354.24. Our future minimum lease payments under the amended operating lease are as follows:
|
Year Ending December 31,
|
|
|
|
|
|
2014
|
|
$
|
220,085
|
|
|
2015
|
|
|
269,844
|
|
|
2016
|
|
|
277,509
|
|
|
2017
|
|
|
285,404
|
|
|
2018
|
|
|
293,537
|
|
|
2019
|
|
|
98,758
|
|
|
TOTAL
|
|
$
|
1,445,137
|
|
Critical Accounting Policies and Estimates
Our discussion and analysis of our financial condition and results of operations are based on our consolidated financial statements, which have been prepared in accordance with accounting principles generally accepted in the United States of America. The preparation of these financial statements requires us to make estimates and judgments that affect the reported amounts of assets, liabilities and expenses. We evaluate our estimates and judgments on an ongoing basis. We base our estimates on historical experience and on assumptions that we believe to be reasonable under the circumstances, the results of which form the basis for making judgments about the carrying values of assets and liabilities that are not readily apparent from other sources. Actual results may differ from these estimates.
We believe the following critical accounting policies affect our more significant judgments and estimates used in the preparation of our consolidated financial statements.
Research and Development. Tonix outsources its research and development efforts and expenses related costs as incurred, including the cost of manufacturing product for testing, licensing fees and costs associated with planning and conducting clinical trials. The value ascribed to patents and other intellectual property acquired was expensed as research and development costs, as it related to particular research and development projects and had no alternative future uses.
Stock Based Compensation. All stock-based payments to employees and to nonemployee directors for their services as directors consisted of grants of restricted stock and stock options, which are measured at fair value on the grant date and recognized in the consolidated statements of operations as compensation expense over the relevant vesting period. Restricted stock payments to nonemployees are recognized as an expense over the period of performance. Such payments are measured at fair value at the earlier of the date a performance commitment is reached or the date performance is completed. In addition, for awards that vest immediately and are nonforfeitable, the measurement date is the date the award is issued.
Income Taxes. Deferred income tax assets and liabilities are determined based on the estimated future tax effects of net operating loss and credit carryforwards and temporary differences between the tax basis of assets and liabilities and their respective financial reporting amounts measured at the current enacted tax rates. The Company records an estimated valuation allowance on its deferred income tax assets if it is not more likely than not that these deferred income tax assets will be realized. The Company recognizes a tax benefit from an uncertain tax position only if it is more likely than not that the tax position will be sustained on examination by taxing authorities, based on the technical merits of the position. The tax benefits recognized in the consolidated financial statements from such a position are measured based on the largest benefit that has a greater than 50% likelihood of being realized upon ultimate settlement.
Recent Accounting Pronouncements
There were various updates recently issued, most of which represented technical corrections to the accounting literature or application to specific industries and are not expected to a have a material impact on the Company's consolidated financial position, results of operations or cash flows.
ITEM 7A – QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK
Not required under Regulation S-K for “smaller reporting companies.”
ITEM 8 - FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
|
Report of Independent Registered Public Accounting Firm
|
|
F-2
|
|
|
|
|
|
Consolidated balance sheets as of December 31, 2013 and 2012 |
|
F-3
|
|
|
|
|
|
Consolidated statements of operations for the years ended December 31, 2013 and 2012 and for the period from June 7, 2007 (date of inception) through December 31, 2013 |
|
F-4
|
|
|
|
|
|
Consolidated statements of comprehensive loss for the years ended December 31, 2013 and 2012 and for the period from June 7, 2007 (date of inception) through December 31, 2013 |
|
F-5
|
|
|
|
|
|
Consolidated statements of stockholders’ equity (deficiency) for the years ended December 31, 2013, 2012, 2011, 2010, 2009, 2008 and for the period from June 7, 2007 (date of inception) through December 31, 2007 |
|
F-6 – F-9
|
|
|
|
|
|
Consolidated statements of cash flows for the years ended December 31, 2013 and 2012 and for the period from June 7, 2007 (date of inception) through December 31, 2013 |
|
F-10
|
|
|
|
|
|
Notes to consolidated financial statements
|
|
F-11 – F-24
|
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
The Board of Directors and Stockholders
Tonix Pharmaceuticals Holding Corp.
We have audited the accompanying consolidated balance sheets of Tonix Pharmaceuticals Holding Corp. (a development stage company) (the “Company”) as of December 31, 2013 and 2012, and the related consolidated statements of operations and comprehensive loss, and cash flows for the years then ended and for the period from June 7, 2007 (inception) through December 31, 2013 and the consolidated statements of stockholders’ (deficiency) equity for each of the six years in the period ended December 31, 2013 and for the period from June 7, 2007 (inception) through December 31, 2007. These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. Our audits included consideration of internal control over financial reporting as a basis for designing audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the financial statements referred to above present fairly, in all material respects, the consolidated financial position of Tonix Pharmaceuticals Holding Corp. as of December 31, 2013 and 2012, the consolidated results of its operations, and its cash flows for the years the ended and for the period from June 7, 2007 (inception) through December 31, 2013 and the consolidated changes in stockholders’ (deficiency) equity for each of the six years in in the period ended December 31, 2013 and for the period from June 7, 2007 (inception) through December 31, 2007, in conformity with accounting principles generally accepted in the United States of America.
/s/ EisnerAmper LLP
New York, New York
March 28, 2014
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
CONSOLIDATED BALANCE SHEETS
DECEMBER 31, 2013 AND 2012
(Dollars In Thousands)
|
|
|
2013
|
|
2012
|
|
|
ASSETS
|
|
|
|
|
|
|
|
|
Current assets:
|
|
|
|
|
|
|
|
|
Cash
|
|
$
|
8,202
|
|
$
|
1,785
|
|
|
Prepaid expenses and other
|
|
|
429
|
|
|
225
|
|
|
Total current assets
|
|
|
8,631
|
|
|
2,010
|
|
|
|
|
|
|
|
|
|
|
|
Furniture and equipment, net
|
|
|
45
|
|
|
47
|
|
|
|
|
|
|
|
|
|
|
|
Restricted cash
|
|
|
60
|
|
|
60
|
|
|
|
|
|
|
|
|
|
|
|
Total assets
|
|
$
|
8,736
|
|
$
|
2,117
|
|
|
|
|
|
|
|
|
|
|
|
LIABILITIES AND STOCKHOLDERS' EQUITY
|
|
|
|
|
|
|
|
|
Current liabilities:
|
|
|
|
|
|
|
|
|
Accounts payable, including $46 and $7 to related parties as of December 31, 2013 and 2012, respectively
|
|
$
|
765
|
|
$
|
825
|
|
|
Accrued expenses, including $491 and $21 to related parties as of December 31, 2013 and 2012, respectively
|
|
|
1,166
|
|
|
310
|
|
|
Promissory notes, related party
|
|
|
280
|
|
|
-
|
|
|
Accrued interest, related party
|
|
|
-
|
|
|
3
|
|
|
Total current liabilities
|
|
|
2,211
|
|
|
1,138
|
|
|
|
|
|
|
|
|
|
|
|
Deferred rent payable
|
|
|
13
|
|
|
20
|
|
|
|
|
|
|
|
|
|
|
|
Total liabilities
|
|
|
2,224
|
|
|
1,158
|
|
|
|
|
|
|
|
|
|
|
|
Commitments (Note 12)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Stockholders' equity:
|
|
|
-
|
|
|
-
|
|
|
Preferred stock, $0.001 par value; 5,000,000 shares authorized, none issued or outstanding
|
|
|
-
|
|
|
-
|
|
|
Common stock, $0.001 par value; 150,000,000 shares authorized; 5,823,081 and 2,159,159 shares issued and outstanding as of December 31, 2013 and 2012, respectively, and 11,002 shares to be issued as of December 31, 2013
|
|
|
6
|
|
|
2
|
|
|
Additional paid in capital
|
|
|
33,235
|
|
|
16,801
|
|
|
Deficit accumulated during development stage
|
|
|
(26,728)
|
|
|
(15,844)
|
|
|
Accumulated other comprehensive loss
|
|
|
(1)
|
|
|
-
|
|
|
|
|
|
|
|
|
|
|
|
Total stockholders' equity
|
|
|
6,512
|
|
|
959
|
|
|
|
|
|
|
|
|
|
|
|
Total liabilities and stockholders' equity
|
|
$
|
8,736
|
|
$
|
2,117
|
|
See the accompanying notes to the consolidated financial statements
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
CONSOLIDATED STATEMENTS OF OPERATIONS
(dollars in thousands, except per share amounts)
|
|
|
|
|
|
|
|
|
From June 7, 2007
|
|
|
|
|
|
|
|
|
|
|
(date of inception)
|
|
|
|
|
Year ended December 31,
|
|
Through
|
|
|
|
|
2013
|
|
2012
|
|
December 31, 2013
|
|
|
COSTS AND EXPENSES:
|
|
|
|
|
|
|
|
|
|
|
|
Research and development
|
|
$
|
4,650
|
|
$
|
2,584
|
|
$
|
9,185
|
|
|
General and administrative
|
|
|
6,238
|
|
|
4,078
|
|
|
14,572
|
|
|
|
|
|
10,888
|
|
|
6,662
|
|
|
23,757
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Operating Loss
|
|
|
(10,888)
|
|
|
(6,662)
|
|
|
(23,757)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Gain on extinguishment of debt
|
|
|
-
|
|
|
-
|
|
|
8
|
|
|
Other income
|
|
|
-
|
|
|
2
|
|
|
2
|
|
|
Change in fair value of warrant liability
|
|
|
-
|
|
|
(1,177)
|
|
|
(1,177)
|
|
|
Interest and other financing costs, net
|
|
|
4
|
|
|
(1,613)
|
|
|
(1,804)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NET LOSS
|
|
$
|
(10,884)
|
|
$
|
(9,450)
|
|
$
|
(26,728)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Net loss per common share, basic and diluted
|
|
$
|
(3.37)
|
|
$
|
(5.58)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Weighted average common shares outstanding, basic and diluted
|
|
|
3,231,311
|
|
|
1,693,416
|
|
|
|
|
See the accompanying notes to the consolidated financial statements
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
CONSOLIDATED STATEMENTS OF COMPREHENSIVE LOSS
(dollars in thousands, except per share amounts)
|
|
|
|
|
|
|
|
|
|
From June 7, 2007
|
|
|
|
|
|
|
|
|
|
|
|
(date of inception)
|
|
|
|
|
Year ended December 31,
|
|
|
Through
|
|
|
|
|
2013
|
|
2012
|
|
December 31, 2013
|
|
|
Net loss
|
|
$
|
(10,884)
|
|
$
|
(9,450)
|
|
$
|
(26,728)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other comprehensive loss:
|
|
|
|
|
|
|
|
|
|
|
|
Foreign currency translation loss
|
|
|
(1)
|
|
|
-
|
|
|
(1)
|
|
|
Total other comprehensive loss
|
|
|
(1)
|
|
|
-
|
|
|
(1)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Comprehensive loss
|
|
$
|
(10,885)
|
|
$
|
(9,450)
|
|
$
|
(26,729)
|
|
See the accompanying notes to the consolidated financial statements
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
CONSOLIDATED STATEMENT OF STOCKHOLDERS' EQUITY (DEFICIENCY)
(dollars in thousands)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accumulated
|
|
Deficit
Accumulated
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Additional
|
|
Other
|
|
During
|
|
|
|
|
|
|
Preferred stock
|
|
Common stock
|
|
Paid in
|
|
Comprehensive
|
|
Development
|
|
|
|
|
|
|
Shares
|
|
Amount
|
|
Shares
|
|
Amount
|
|
Capital
|
|
Loss
|
|
Stage
|
|
Total
|
|
|
Shares issued to founders for intellectual property in June 2007 ($3.00 per share)
|
|
-
|
|
$
|
-
|
|
29,451
|
|
$
|
-
|
|
$
|
88
|
|
$
|
-
|
|
$
|
-
|
|
$
|
88
|
|
|
Shares issued to bankers for services in June 2007 ($3.00 per share)
|
|
-
|
|
|
-
|
|
3,272
|
|
|
-
|
|
|
10
|
|
|
-
|
|
|
-
|
|
|
10
|
|
|
Compensation related to restricted share awards issued to directors in November 2007
|
|
-
|
|
|
-
|
|
-
|
|
|
-
|
|
|
24
|
|
|
-
|
|
|
-
|
|
|
24
|
|
|
Net loss
|
|
-
|
|
|
-
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
(537)
|
|
|
(537)
|
|
|
Balance at December 31, 2007
|
|
-
|
|
|
-
|
|
32,723
|
|
|
-
|
|
|
122
|
|
|
-
|
|
|
(537)
|
|
|
(415)
|
|
|
Compensation related to cancelled restricted share awards in December 2008
|
|
-
|
|
|
-
|
|
-
|
|
|
-
|
|
|
72
|
|
|
-
|
|
|
-
|
|
|
72
|
|
|
Net loss
|
|
-
|
|
|
-
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
(202)
|
|
|
(202)
|
|
|
Balance at December 31, 2008
|
|
-
|
|
|
-
|
|
32,723
|
|
|
-
|
|
|
194
|
|
|
-
|
|
|
(739)
|
|
|
(545)
|
|
|
Conversion of senior convertible notes into Preferred stock in June 2009 ($2.60 per share)
|
|
-
|
|
|
-
|
|
360,005
|
|
|
1
|
|
|
200
|
|
|
-
|
|
|
-
|
|
|
201
|
|
|
Shares issued to directors in July 2009 ($3.00 per share)
|
|
-
|
|
|
-
|
|
1,571
|
|
|
-
|
|
|
4
|
|
|
-
|
|
|
-
|
|
|
4
|
|
|
Capital contribution in June 2009
|
|
-
|
|
|
-
|
|
-
|
|
|
-
|
|
|
24
|
|
|
-
|
|
|
-
|
|
|
24
|
|
|
Net loss
|
|
-
|
|
|
-
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
(221)
|
|
|
(221)
|
|
|
Balance at December 31, 2009
|
|
-
|
|
$
|
-
|
|
394,299
|
|
$
|
1
|
|
$
|
422
|
|
$
|
-
|
|
$
|
(960)
|
|
$
|
(537)
|
|
See the accompanying notes to the consolidated financial statements
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
CONSOLIDATED STATEMENT OF STOCKHOLDERS' EQUITY (DEFICIENCY)
(dollars in thousands)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accumulated
|
|
Deficit
Accumulated
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Additional
|
|
Other
|
|
During
|
|
|
|
|
|
|
|
Preferred stock
|
|
Common stock
|
|
Paid in
|
|
Comprehensive
|
|
Development
|
|
|
|
|
|
|
|
Shares
|
|
Amount
|
|
Shares
|
|
Amount
|
|
Capital
|
|
Loss
|
|
Stage
|
|
Total
|
|
|
Conversion of demand notes into capital stock in July 2010 ($4.60 per share)
|
|
-
|
|
$
|
-
|
|
104,729
|
|
$
|
-
|
|
$
|
480
|
|
$
|
-
|
|
$
|
-
|
|
$
|
480
|
|
|
Conversion of accrued interest on demand notes into capital stock in July 2010 ($4.60 per share)
|
|
-
|
|
|
-
|
|
15,072
|
|
|
-
|
|
|
69
|
|
|
-
|
|
|
-
|
|
|
69
|
|
|
Issuance of capital stock in August to December 2010 ($4.60 per share)
|
|
-
|
|
|
-
|
|
292,805
|
|
|
-
|
|
|
1,342
|
|
|
-
|
|
|
-
|
|
|
1,342
|
|
|
Shares issued to founders for intellectual property in June 2010 ($4.52 per share)
|
|
-
|
|
|
-
|
|
65,447
|
|
|
-
|
|
|
295
|
|
|
-
|
|
|
-
|
|
|
295
|
|
|
Issuance of restricted shares to directors, employees and consultants in June to November 2010 ($4.76 per share)
|
|
-
|
|
|
-
|
|
29,385
|
|
|
-
|
|
|
140
|
|
|
-
|
|
|
-
|
|
|
140
|
|
|
Net loss
|
|
-
|
|
|
-
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
(1,964)
|
|
|
(1,964)
|
|
|
Balance at December 31, 2010
|
|
-
|
|
|
-
|
|
901,737
|
|
|
1
|
|
|
2,748
|
|
|
-
|
|
|
(2,924)
|
|
|
(175)
|
|
|
Vesting and issuance of capital stock in January to September 2011 ($4.60 per share)
|
|
-
|
|
|
-
|
|
133,530
|
|
|
-
|
|
|
612
|
|
|
-
|
|
|
-
|
|
|
612
|
|
|
Vesting and issuance of restricted shares to directors, employees and consultants in February to April 2011 and vesting of restricted shares pursuant to share exchange in October 2011 ($4.60 per share)
|
|
-
|
|
|
-
|
|
98,084
|
|
|
-
|
|
|
435
|
|
|
-
|
|
|
-
|
|
|
435
|
|
|
Common stock issued in connection with the share exchange transaction in October 2011
|
|
-
|
|
|
-
|
|
200,000
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
Common stock issued in October 2011 in exchange for services rendered ($7.20 per share)
|
|
-
|
|
|
-
|
|
20,000
|
|
|
-
|
|
|
144
|
|
|
-
|
|
|
-
|
|
|
144
|
|
|
Net loss
|
|
-
|
|
|
-
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
(3,470)
|
|
|
(3,470)
|
|
|
Balance at December 31, 2011
|
|
-
|
|
$
|
-
|
|
1,353,351
|
|
$
|
1
|
|
$
|
3,939
|
|
$
|
-
|
|
$
|
(6,394)
|
|
$
|
(2,454)
|
|
See the accompanying notes to the consolidated financial statements
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
CONSOLIDATED STATEMENT OF STOCKHOLDERS' EQUITY (DEFICIENCY)
(dollars in thousands)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accumulated
|
|
Deficit
Accumulated
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Additional
|
|
Other
|
|
During
|
|
|
|
|
|
|
Preferred stock
|
Common stock
|
|
Paid in
|
|
Comprehensive
|
|
Development
|
|
|
|
|
|
|
|
Shares
|
|
Amount
|
|
Shares
|
|
Amount
|
|
Capital
|
|
Loss
|
|
Stage
|
|
Total
|
|
|
Issuance of common stock in January 2012 to holders of convertible debentures ($12.40 per share)
|
|
|
-
|
|
$
|
-
|
|
|
29,700
|
|
$
|
-
|
|
$
|
369
|
|
$
|
-
|
|
$
|
-
|
|
$
|
369
|
|
|
Issuance of common stock in January and March 2012 ( $12.40 per share) net of transaction expenses of $436
|
|
|
-
|
|
|
-
|
|
|
330,893
|
|
|
1
|
|
|
3,632
|
|
|
-
|
|
|
-
|
|
|
3,633
|
|
|
Warrants issued in January 2012 to holders of convertible debentures
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
83
|
|
|
-
|
|
|
-
|
|
|
83
|
|
|
Warrants issued to placement agent in January 2012
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
6
|
|
|
-
|
|
|
-
|
|
|
6
|
|
|
Warrants reclassified to equity upon expiry of reset provisions
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
3,939
|
|
|
-
|
|
|
-
|
|
|
3,939
|
|
|
Issuance of common stock and warrants in December 2012 to holders of convertible debentures ($6.00 per share)
|
|
|
-
|
|
|
-
|
|
|
118,335
|
|
|
-
|
|
|
710
|
|
|
-
|
|
|
-
|
|
|
710
|
|
|
Issuance of common stock and warrants in December 2012 ($8.00 per share) net of transaction expenses of $70
|
|
|
-
|
|
|
-
|
|
|
326,879
|
|
|
-
|
|
|
2,545
|
|
|
-
|
|
|
-
|
|
|
2,545
|
|
|
Beneficial conversion feature in connection with convertible debentures
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
710
|
|
|
-
|
|
|
-
|
|
|
710
|
|
|
Capital contribution of accrued interest
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
3
|
|
|
-
|
|
|
-
|
|
|
3
|
|
|
Stock based compensation
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
865
|
|
|
-
|
|
|
-
|
|
|
865
|
|
|
Net loss
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
(9,450)
|
|
|
(9,450)
|
|
|
Balance at December 31, 2012
|
|
|
-
|
|
$
|
-
|
|
|
2,159,159
|
|
$
|
2
|
|
$
|
16,801
|
|
$
|
-
|
|
$
|
(15,844)
|
|
$
|
959
|
|
See the accompanying notes to the consolidated financial statements
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
CONSOLIDATED STATEMENT OF STOCKHOLDERS' EQUITY (DEFICIENCY)
(dollars in thousands)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accumulated
|
|
Deficit
Accumulated
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Additional
|
|
Other
|
|
During
|
|
|
|
|
|
|
Preferred stock
|
Common stock
|
|
Paid in
|
|
Comprehensive
|
|
Development
|
|
|
|
|
|
|
|
Shares
|
|
Amount
|
|
Shares
|
|
Amount
|
|
Capital
|
|
Loss
|
|
Stage
|
|
Total
|
|
|
Stock based compensation
|
|
|
-
|
|
$
|
-
|
|
|
-
|
|
$
|
-
|
|
$
|
1,717
|
|
$
|
-
|
|
$
|
-
|
|
$
|
1,717
|
|
|
Issuance of common stock in exchange for exercise of warrants in April 2013 ($8.00 per share)
|
|
|
-
|
|
|
-
|
|
|
38,334
|
|
|
-
|
|
|
307
|
|
|
-
|
|
|
-
|
|
|
307
|
|
|
Issuance of common stock and warrants in August 2013 ($4.25 per share) net of transaction expenses of $1,352
|
|
|
-
|
|
|
-
|
|
|
2,680,000
|
|
|
3
|
|
|
10,039
|
|
|
-
|
|
|
-
|
|
|
10,042
|
|
|
Common stock issued (873,885) or to be issued (11,002) in exchange for exercise of warrants in December 2013 ($4.25 per share)
|
|
|
-
|
|
|
-
|
|
|
884,887
|
|
|
1
|
|
|
3,760
|
|
|
-
|
|
|
-
|
|
|
3,761
|
|
|
Issuance of common stock in exchange for exercise of warrants in December 2013 ($8.00 per share)
|
|
|
-
|
|
|
-
|
|
|
70,031
|
|
|
-
|
|
|
560
|
|
|
-
|
|
|
-
|
|
|
560
|
|
|
Issuance of common stock in exchange for 3,185 warrants exercised on a cashless basis
|
|
|
-
|
|
|
-
|
|
|
1,672
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
Warrants issued for services rendered
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
51
|
|
|
-
|
|
|
-
|
|
|
51
|
|
|
Foreign currency translation adjustment
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
(1)
|
|
|
-
|
|
|
(1)
|
|
|
Net loss
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
(10,884)
|
|
|
(10,884)
|
|
|
Balance at December 31, 2013
|
|
|
-
|
|
$
|
-
|
|
|
5,834,083
|
|
$
|
6
|
|
$
|
33,235
|
|
$
|
(1)
|
|
$
|
(26,728)
|
|
$
|
6,512
|
|
See the accompanying notes to the consolidated financial statements
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
CONSOLIDATED STATEMENTS OF CASH FLOWS
(dollars in thousands)
|
|
|
|
|
|
|
|
|
From June 7, 2007
|
|
|
|
|
|
|
|
|
|
|
(date of inception)
|
|
|
|
|
Year ended December 31,
|
|
Through
|
|
|
|
|
2013
|
|
2012
|
|
December 31, 2013
|
|
|
CASH FLOWS FROM OPERATING ACTIVITIES:
|
|
|
|
|
|
|
|
|
|
|
|
Net loss
|
|
$
|
(10,884)
|
|
$
|
(9,450)
|
|
$
|
(26,728)
|
|
|
Adjustments to reconcile net loss to net cash used in operating activities:
|
|
|
|
|
|
|
|
|
|
|
|
Depreciation
|
|
|
17
|
|
|
14
|
|
|
49
|
|
|
Amortization and write off of deferred financing costs
|
|
|
-
|
|
|
196
|
|
|
250
|
|
|
Non cash interest, consisting of beneficial conversion feature in connection with convertible debentures
|
|
|
-
|
|
|
710
|
|
|
710
|
|
|
Non cash interest, consisting of common stock and warrants issued in connection with convertible debentures
|
|
|
-
|
|
|
426
|
|
|
426
|
|
|
Non-cash financing costs related to January and March 2012 financing
|
|
|
-
|
|
|
81
|
|
|
81
|
|
|
Warrants issued for services rendered
|
|
|
51
|
|
|
-
|
|
|
51
|
|
|
Stock based compensation
|
|
|
1,717
|
|
|
865
|
|
|
3,269
|
|
|
Change in fair value of warrant liability
|
|
|
-
|
|
|
1,177
|
|
|
1,177
|
|
|
Common stock issued in exchange for intellectual property
|
|
|
-
|
|
|
-
|
|
|
383
|
|
|
Gain on extinguishment of debt
|
|
|
-
|
|
|
-
|
|
|
(8)
|
|
|
Changes in operating assets and liabilities:
|
|
|
|
|
|
|
|
|
|
|
|
Prepaid expenses
|
|
|
(204)
|
|
|
(122)
|
|
|
(429)
|
|
|
Accounts payable
|
|
|
(60)
|
|
|
132
|
|
|
766
|
|
|
Accrued interest
|
|
|
(3)
|
|
|
(32)
|
|
|
3
|
|
|
Accrued expenses
|
|
|
856
|
|
|
293
|
|
|
1,260
|
|
|
Deferred rent payable
|
|
|
(7)
|
|
|
(3)
|
|
|
19
|
|
|
Net cash used in operating activities
|
|
|
(8,517)
|
|
|
(5,713)
|
|
|
(18,721)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CASH FLOWS FROM INVESTING ACTIVITIES:
|
|
|
|
|
|
|
|
|
|
|
|
Purchase of furniture and fixtures
|
|
|
(15)
|
|
|
(36)
|
|
|
(94)
|
|
|
Payment of restricted cash and interest earned on restricted cash
|
|
|
-
|
|
|
-
|
|
|
(60)
|
|
|
Net cash used in investing activities
|
|
|
(15)
|
|
|
(36)
|
|
|
(154)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CASH FLOWS FROM FINANCING ACTIVITIES:
|
|
|
|
|
|
|
|
|
|
|
|
Proceeds from demand notes
|
|
|
-
|
|
|
-
|
|
|
480
|
|
|
Proceeds from other notes payable
|
|
|
-
|
|
|
320
|
|
|
1,020
|
|
|
Proceeds from related party promissory notes
|
|
|
280
|
|
|
-
|
|
|
280
|
|
|
Proceeds from exercise of warrants
|
|
|
4,628
|
|
|
-
|
|
|
4,628
|
|
|
Proceeds, net of expenses of $24 as of December 31, 2011 from Convertible Debentures
|
|
|
-
|
|
|
390
|
|
|
1,891
|
|
|
Repayment of Convertible Debentures
|
|
|
-
|
|
|
(150)
|
|
|
(150)
|
|
|
Proceeds, net of expenses of $1,352 (2013) and $506 (2012), from sale of units consisting of common stock and warrants
|
|
|
10,042
|
|
|
6,933
|
|
|
16,975
|
|
|
Proceeds from the sale of capital stock
|
|
|
-
|
|
|
-
|
|
|
1,954
|
|
|
Net cash provided by financing activities
|
|
|
14,950
|
|
|
7,493
|
|
|
27,078
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Effect of currency rate change on cash
|
|
|
(1)
|
|
|
-
|
|
|
(1)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Net increase in cash
|
|
|
6,417
|
|
|
1,744
|
|
|
8,202
|
|
|
Cash, beginning of the period
|
|
|
1,785
|
|
|
41
|
|
|
-
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cash, end of period
|
|
$
|
8,202
|
|
$
|
1,785
|
|
$
|
8,202
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Supplemental disclosures of cash flow information:
|
|
|
|
|
|
|
|
|
|
|
|
Interest paid
|
|
$
|
3
|
|
$
|
35
|
|
$
|
38
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Non cash investing and financing activities:
|
|
|
|
|
|
|
|
|
|
|
|
Senior convertible notes exchanged for preferred shares
|
|
$
|
-
|
|
$
|
-
|
|
$
|
200
|
|
|
Capital contribution of accrued interest
|
|
$
|
-
|
|
$
|
-
|
|
$
|
27
|
|
|
Demand notes together with accrued interest converted into capital stock
|
|
$
|
-
|
|
$
|
-
|
|
$
|
549
|
|
|
Common stock issued for deferred financing costs
|
|
$
|
-
|
|
$
|
-
|
|
$
|
144
|
|
|
Exchange of Notes Payable for Convertible Debenture
|
|
$
|
-
|
|
$
|
320
|
|
$
|
820
|
|
|
Warrants Liability reclassified to Stockholders' Equity
|
|
$
|
-
|
|
$
|
3,939
|
|
$
|
3,939
|
|
|
Exchange of Convertible Debenture for Units consisting of common stock and warrants
|
|
$
|
-
|
|
$
|
2,635
|
|
$
|
2,635
|
|
See the accompanying notes to consolidated financial statements
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 1 – BUSINESS
Tonix Pharmaceuticals Holding Corp., through its wholly owned subsidiary Tonix Pharmaceuticals, Inc., or Tonix Sub, is a specialty pharmaceutical company dedicated to the identification and development of novel pharmaceutical products for challenging disorders of the central nervous system (“CNS”).
On October 24, 2013, Tonix Sub formed Tonix Pharmaceuticals (Barbados), Ltd. (“Tonix Barbados”). On December 31, 2013 Tonix Barbados entered into a license agreement and a cost-sharing agreement with Tonix Sub, pursuant to which Tonix Barbados acquired the rights to develop and commercialize certain products (TNX-102 SL and TNX-201) for non-US markets.
On April 23, 2013, Tonix Sub formed a wholly owned subsidiary, Tonix Pharmaceuticals (Canada), Inc., in the province of New Brunswick, Canada for the purpose of obtaining research and development credits from the Canadian government for any research and development studies performed in Canada.
On August 16, 2010, Tonix Pharmaceuticals, Inc. formed Krele LLC ("Krele") in the state of Delaware. Krele is a limited liability corporation whose sole member is Tonix Pharmaceuticals Inc. Krele was established to commercialize products that are generic versions of predicate new drug application products or versions of drug efficacy study implementation products. Tonix Pharmaceuticals, Inc. expects that its relationship to Krele will be similar to that of several other pharmaceutical companies and their subsidiaries that market generic versions of the parent's branded products at different periods in their product life-cycle.
NOTE 2 – SIGNIFICANT ACCOUNTING POLICIES
Consolidation
The consolidated financial statements include the accounts of Tonix Pharmaceuticals Holding Corp. and its wholly owned subsidiaries, Tonix Pharmaceuticals, Inc., Krele LLC, Tonix Pharmaceuticals (Canada), Inc., and Tonix Pharmaceuticals (Barbados), Ltd. (hereafter referred to as the “Company” or “Tonix”).
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
All significant intercompany balances and transactions have been eliminated in consolidation.
Development Stage
As the Company is devoting substantially all of its efforts to establishing a new business, and while planned principal operations have commenced, there has been no revenue generated from sales, license fees or royalties, the Company is considered a development stage enterprise. Accordingly, the Company's consolidated financial statements are presented in accordance with authoritative accounting guidance related to a development stage enterprise. Financial position, results of operations and cash flows of a development stage enterprise are presented in conformity with generally accepted accounting principles that apply to established operating enterprises.
Liquidity
As a development stage enterprise, the Company's primary efforts are devoted to conducting research and development for the treatment of CNS diseases. The Company has experienced net losses and negative cash flows from operations since inception and expects these conditions to continue for the foreseeable future. Further, the Company does not have any commercial products available for sale and has not generated revenues and there is no assurance that if approval of their products is received that the Company will be able to generate cash flow to fund operations. In addition, there can be no assurance that the Company's research and development will be successfully completed or that any product will be approved or commercially viable.
At December 31, 2013, the Company has working capital of approximately $7,000,000 attributable to the sale of units consisting of common stock and warrants in August 2013 and receiving net proceeds of approximately $10,000,000. In addition, in the first quarter of 2014, the Company raised approximately $40.7 million through the sale of common stock in an underwritten public offering and approximately $4.8 million upon the exercise of previously issued warrants (see Note 15). Management believes that the Company has sufficient funds to meet its research and development and other funding requirements for at least the next twelve months. The Company expects that cash used in operations will increase significantly over the next several years. In the event the funding obtained is not sufficient to complete the development and commercialization of its current product candidates, the Company intends to raise additional funds through equity or debt financing. If the Company is unsuccessful in raising additional financing, it will need to reduce costs and operations in the future.
Use of estimates
The preparation of financial statements in accordance with accounting principles generally accepted in the United States requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosures of contingent assets and liabilities at the date of the financial statements, and the reported amounts of revenues and expenses during the reporting period. Actual results could differ from those estimates. Significant estimates include the useful life of fixed assets, assumptions used in the fair value of stock-based compensation and other equity instruments, and the percent of completion of research and development contracts.
Research and Development costs
The Company outsources its research and development efforts and expenses related costs as incurred, including the cost of manufacturing product for testing, as well as licensing fees and costs associated with planning and conducting clinical trials. The value ascribed to patents and other intellectual property acquired was expensed in 2007 and 2010 as research and development costs, as it related to particular research and development projects and had no alternative future uses.
Furniture and equipment
Furniture and equipment are stated at cost, less accumulated depreciation. Depreciation is calculated using the straight-line method over the asset's estimated useful life, which is three years for computer assets and five years for furniture and all other equipment. Expenditures for maintenance and repairs are expensed as incurred.
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
Income taxes
Deferred income tax assets and liabilities are determined based on the estimated future tax effects of net operating loss and credit carryforwards and temporary differences between the tax basis of assets and liabilities and their respective financial reporting amounts measured at the current enacted tax rates. The Company records an estimated valuation allowance on its deferred income tax assets if it is not more likely than not that these deferred income tax assets will be realized.
The Company recognizes a tax benefit from an uncertain tax position only if it is more likely than not that the tax position will be sustained on examination by taxing authorities, based on the technical merits of the position. The tax benefits recognized in the consolidated financial statements from such a position are measured based on the largest benefit that has a greater than 50% likelihood of being realized upon ultimate settlement. As of December 31, 2013 and 2012, the Company has not recorded any unrecognized tax benefits.
Stock-based compensation
All stock-based payments to employees and to nonemployee directors for their services as directors, including grants of restricted stock and stock options, are measured at fair value on the grant date and recognized in the consolidated statements of operations as compensation or other expense over the relevant service period. Stock-based payments to nonemployees are recognized as an expense over the period of performance. Such payments are measured at fair value at the earlier of the date a performance commitment is reached or the date performance is completed. In addition, for awards that vest immediately and are non-forfeitable the measurement date is the date the award is issued.
Foreign Currency Translation
Operations of the Canadian subsidiary are conducted in local currency which represents its functional currency. Balance sheet accounts of such subsidiary were translated from foreign currency into U.S. dollars at the exchange rate in effect at the balance sheet date and income statement accounts were translated at the average rate of exchange prevailing during the period. Translation adjustments resulting from this process, were included in accumulated other comprehensive loss on the consolidated balance sheet.
Comprehensive Income (Loss)
The Company adopted authoritative guidance issued by the Financial Accounting Standards Board which establishes standards for the reporting and displaying of comprehensive income (loss) and its components and elected to present comprehensive loss and net loss in two separate but consecutive statements. Comprehensive income (loss) is defined as the change in equity of a business during a period from transactions and other events and circumstances from non-owners sources. It includes all changes in equity during a period except those resulting from investments by owners and distributions to owners. Other comprehensive loss represents foreign currency translation adjustments.
Per share data
Basic and diluted net loss per common share is calculated by dividing net loss, by the weighted average number of outstanding shares of common stock, adjusted to give effect to the 20-for-1 reverse stock split, which was effected on May 1, 2013 (see Note 9).
As of December 31, 2013 and 2012, there were outstanding warrants to purchase an aggregate of 3,137,656 and 1,259,934 shares, respectively, of the Company’s common stock (see Note 11). In addition, the Company has issued to employees, options to acquire shares of the Company’s common stock of which 376,500 and 150,000 were outstanding at December 31, 2013 and 2012, respectively (see Note 10). In computing diluted net loss per share for the years ended December 31, 2013 and 2012, no effect has been given to such options and warrants as their effect would be anti-dilutive.
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 3 – FURNITURE AND EQUIPMENT
Furniture and equipment as of December 31, 2013 and 2012 is summarized as follows:
|
|
|
2013
|
|
2012
|
|
|
Office furniture and equipment
|
|
$
|
93,188
|
|
$
|
78,535
|
|
|
Less: accumulated depreciation
|
|
|
(48,232)
|
|
|
(31,641)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$
|
44,956
|
|
$
|
46,894
|
|
Depreciation expense for the years ended December 31, 2013 and 2012 was $16,591 and $14,329, respectively.
NOTE 4 – RESTRICTED CASH
Restricted cash at December 31, 2013 and 2012 collateralizes a letter of credit in the amount of approximately $60,000 issued in connection with the lease of office space in New York City (see Note 12).
NOTE 5 – AUGUST 2013 FINANCING
On August 9, 2013, the Company entered into an underwriting agreement (the “Underwriting Agreement”) with Roth Capital Partners, LLC, as representative of the underwriters named therein (the “Underwriters”), pursuant to which the Company agreed to offer to the public through the Underwriters an aggregate of 2,680,000 units (each a “Unit”, and collectively, the “Units”) at a public offering price of $4.25 per Unit in an underwritten public offering (the “August 2013 Financing”). Each Unit consisted of (i) one share of common stock and (ii) one Series A Warrant (the “Warrants”) to purchase one share of common stock. The Warrants are exercisable at an exercise price of $4.25 per share, subject to anti-dilutive adjustment, and expire on the fifth anniversary of the date of issuance. The Warrants will be exercisable on a “cashless” basis in certain circumstances. Pursuant to the Underwriting Agreement, the Company also granted the Underwriters an option for a period of 45 days to purchase up to (i) 402,000 additional Units or (ii) 402,000 additional shares of common stock and/or additional Warrants to purchase up to 402,000 shares of common stock, on the same terms, to cover over-allotments, if any.
The August 2013 Financing closed on August 14, 2013. The Underwriters purchased the Units at an eight-percent discount to the public offering price, for an aggregate discount of approximately $911,200 (or $0.34 per unit). The Company received net cash proceeds of $10,038,013 after deducting underwriting discounts and commissions and offering expenses of $440,787. On August 14, 2013, the Underwriters exercised their over-allotment option by purchasing for $4,020 additional Warrants to purchase 402,000 shares of common stock.
The Underwriters received warrants to purchase up to an aggregate of 107,200 shares of common stock, or four percent of the total number of shares included in the Units, which warrants have an exercise price of $4.25.
NOTE 6 – JANUARY AND MARCH 2012 FINANCING
On January 20, 2012, the Company issued an aggregate of 172.118 units (“Units”) to certain investors (the “Purchasers”) for aggregate cash proceeds of $2,377,950 and $1,925,000 in previously issued Convertible Debentures of the Company that were exchanged for Units (“January 2012 Financing”). On March 1, 2012, the Company issued an aggregate of 92.5926 units to certain investors for aggregate cash proceeds of $2,314,815 (“March 2012 Financing”).
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
Each Unit had a purchase price of $25,000 per Unit and consisted of 1,250 shares of the Company’s common stock, a Class A Warrant to purchase 1,250 shares of Common Stock (the “Class A Warrants”), and a Class B Warrant to purchase up to 1,250 shares of Common Stock (the “Class B Warrants” and together with the Class A Warrants, the “Warrants”).
The Class A Warrants have an exercise price of $25.00 per share of common stock and will be exercisable for a period of five years from the date of issuance. The warrants had certain anti-dilutive provisions that were set to expire the earlier of i) one year or ii) upon effectiveness of a registration of all shares covered by Class A Warrants, which took place on June 6, 2012. The Company determined the fair value of the Class A Warrants and the Agent Warrants, described below, to be $2,549,684 and $212,235 on the issuance dates and initially classified them as a liability due to transactions which cause an adjustment to the conversion rate (reset provisions) contained in the warrant agreements. On June 6, 2012, upon the Company's registration statement being declared effective by the Securities and Exchange Commission, the reset provisions expired and the Company reclassified $3,938,946, the fair value of the Class A Warrants and Agent Warrants as of that date to equity. The increase of $1,177,026 in fair value of warrants liability was included in results of operations for the year ended December 31, 2012.
The following assumptions were used in the Binomial Lattice model to determine fair value of the Class A Warrants and the Agent Warrants:
|
|
|
Issuance date
January 20 and
March 1, 2012
|
|
|
Expiration date
June 6, 2012
|
|
|
Price of the Company’s common stock
|
|
$
|
12.40
|
|
|
$
|
17.00
|
|
|
Dividend yield
|
|
|
0
|
%
|
|
|
0
|
%
|
|
Expected terms
|
|
|
5 – 7 years
|
|
|
|
4.6 - 6.7 years
|
|
|
Risk free interest rate
|
|
|
0.89 - 1.47
|
%
|
|
|
0.73 - 1.11
|
%
|
|
Expected volatility
|
|
|
96.68 - 96.69
|
%
|
|
|
95.73
|
%
|
|
Expected price at which holders are likely to exercise their warrants
|
|
$
|
25.00
|
|
|
$
|
25.00
|
|
The Class B Warrants were exercisable automatically on their expiration date by cashless exercise or expire without exercise. In the event that the average of the Company’s daily volume weighted average price was below $15.00 during the 10 trading days after the Announcement Date (as hereinafter defined) (the “Measuring Period”), then the holder was entitled to receive additional shares of the Company’s Common Stock upon the exercise of the Class B Warrants on the expiration date, which is the 12th trading day after the Announcement Date. In the event that the Company’s average daily volume weighted average price was at or above $15.00 during the Measuring Period, the Class B Warrants were to expire unexercised. The Announcement Date was the earlier of (1) the date on which the Company announces via press release the results of the pharmacokinetic study of TNX-102 gelcap; or (2) June 1, 2012. On April 5, 2012 the Company issued a press release announcing the results of the pharmacokinetic study of TNX-102 gelcap, which is defined as an Announcement Date for the purpose of the Class B Warrants. Based on the Company’s average daily volume weighted average price of $34.60 per share during the Measuring Period, the Class B Warrants expired unexercised.
In connection with the January and March 2012 Financing, the Company paid a placement agent (the “Agent”) an aggregate cash payment of $466,777, which represented an 8% commission and a 2% non-accountable expense allowance of the gross proceeds delivered by Purchasers in the January and March 2012 Financing. In addition, the Agent earned an aggregate of 23,339 warrants to purchase shares of common stock equal to 10% of the gross proceeds delivered by Purchasers in the January and March 2012 Financing (the “Agent Warrants”), which have an exercise price of $25.00 per share of common stock, exercisable for a period of seven years, contained anti-dilution protection and are entitled to piggy-back registration rights. Total expenses related to the financing, including cash and the fair value of warrants given to the Agent, amounted to $706,511, of which $435,713 was charged to additional paid-in capital and $270,798, deemed initially allocable to the warrant liability, was charged to interest and other financing costs.
As described above, upon the January 2012 Financing, $1,925,000 Convertible Debentures were exchanged for Units and the remaining $150,000 of debentures were repaid. Upon conversion or repayment of the Convertible Debentures, the holder was entitled to receive, at the holder’s option, either (i) a warrant (the “Debenture Warrant”), which has a three year term and is exercisable at the offering price in a Subsequent Financing, to purchase such number of shares of the Company's common stock equal to the principal amount of the Convertible Debenture divided by the offering price in a Subsequent Financing, (the “Warrant Shares”) or (ii) shares of the Company's common stock equal to 33% of the principal amount of the Convertible Debenture divided by the offering price in a Subsequent Financing (the “Incentive Shares”). Upon the January 2012 Financing, the holders of the Convertible Debenture elected to receive 13,750 Debenture Warrants exercisable at $20.00 per share with a fair value of $83,289 and 29,700 Incentive Shares valued at $368,280. The value of the Debenture Warrants and Incentive Shares was charged to operations as interest expense in the first quarter of 2012.
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
In connection with the financings, the Company entered into a Registration Rights Agreement with Purchasers. The Company was required to file a registration statement registering for resale the common stock included in the Units and the common stock underlying the Class A Warrants and the Agent Warrants to be filed no later than 60 days from the date of termination of the financings on March 1, 2012 and must be declared effective no later than 120 days from the date of termination of the Financing (June 29, 2012). On April 26, 2012, the Company filed the registration statement, which was declared effective on June 6, 2012. The Company is required to maintain the effectiveness of the registration statement from its effective date unless all securities registered under the registration statement have been sold or are otherwise able to be sold. If the Company failed to comply with the registration statement filing or effective date requirements, the Company was required to pay the investors a fee equal to 1.0% of the Purchaser’s investment, for each 30-day period of delay, subject to a maximum payment of 10% to each Purchaser.
NOTE 7 – 2012 CONVERTIBLE DEBENTURES
On November 14, 2012, the Company sold to accredited investors for aggregate cash proceeds of $390,000, convertible debentures (“Debentures”) in the principal face amount of $390,000 and the Company exchanged $320,000 in previously issued promissory notes of the Company for Debentures in the principal face amount of $320,000.
The previously issued promissory notes were issued between October and November 2012 in the amount of $320,000 in exchange for $320,000 borrowed from six affiliated investors. The Notes bore no interest and were payable on demand.
The Debentures mature on the earlier of (i) November 14, 2013 or (ii) the date of closing of a private placement of equity, equity equivalent, convertible debt or debt financing in which we receive gross proceeds, in one or more transactions, of at least $100,000 (a “Subsequent Financing”). The Debentures bear interest at 8% per annum and are convertible at the holder’s option into either (i) a Subsequent Financing at a price equal to a 25% discount to the price of securities sold in the Subsequent Financing or (ii) shares of the Company’s common stock at a conversion price per share equal to $20.00.
On December 4, 2012, upon completion of a Subsequent Financing, the $710,000 of Debentures were converted into Units at a price of $0.30 per Unit representing a 25% discount to the price ($0.40) of securities sold (the “Financing”). Accordingly, the Company recorded a beneficial conversion feature in connection with the Debentures at the date of conversion of $710,000 as a charge to interest expense and a credit to additional paid in capital.
The beneficial conversion feature, which was contingent on a Subsequent Financing, was computed based on the excess of the number of shares received upon conversion based on the adjusted conversion price ($0.30) over the number of shares that would have been received based on the original conversion price ($1.00) multiplied by the stock price of ($0.51) on November 14, 2012, the date the Debentures were issued, limited to the amount of proceeds allocated to the Debentures, or $710,000.
NOTE 8 – DECEMBER 2012 FINANCING
On December 4, 2012, the Company issued an aggregate of 6,404,167 units (“Units”) to certain accredited investors for aggregate cash proceeds of $1,615,000, at a price per Unit of $0.40, and the exchange of $710,000 in previously issued convertible debentures of the Company that were converted into Units at a price of $0.30 per Unit. On December 21, 2012, the Company issued 2,500,000 Units to a single accredited investor for cash proceeds of $1,000,000, at a price per Unit of $0.40. In connection with the Financing, the Company paid an agent a cash payment of $70,000, which represented a 7% commission of the gross proceeds delivered by the investor in the financing.
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
Each Unit consisted of 0.05 share of the Company’s common stock, $0.001 par value, a Class A Warrant to purchase 0.05 share of Common Stock (the “Class A Warrants”), and a Class B Warrant to purchase 0.05 share of Common Stock (the “Class B Warrants” and together with the Class A Warrants, the “Warrants”). The Class A Warrants have an exercise price of $12.00 per share of Common Stock and will be exercisable for a period of five years from the date of issuance. The Class A Warrants may be exercised on a cashless basis under certain circumstances. The Class B Warrants had an exercise price of $8.00 per share of Common Stock and were exercisable for a period of one year from the date of issuance. In December 2013, all unexercised Class B Warrants expired.
In connection with the Financing, the Company granted each Purchaser registration rights. The Company is obligated to use its best efforts to cause a registration statement registering for resale the common stock included in the Units and the common stock underlying the Class A Warrants to be filed no later than 60 days (as amended) from the date of termination of the Financing and must be declared effective no later than 120 days from the date of termination of the Financing. Moreover, the Company will maintain the effectiveness of the registration statement from its effective date unless all securities registered under the registration statement have been sold or are otherwise able to be sold pursuant to Rule 144 of the Securities Act of 1933, as amended. If the Company fails to comply with the registration statement filing or effective date requirements, the Company was required to pay the investors a fee equal to 1.0% of the Purchaser’s investment, for each 30-day period of delay, subject to a maximum payment of 10% to each Purchaser. On January 25, 2013, the Company filed the required registration statement which was declared effective by the Securities and Exchange Commission on April 5, 2013.
NOTE 9 – STOCKHOLDERS' EQUITY
On May 2, 2012, the Company filed amended and restated Articles of Incorporation. Among other changes, the Company increased the number of authorized shares of common stock, $0.001 par value to 150,000,000. Additionally, the Company is now authorized to issue 5,000,000 shares of preferred stock, $0.001 par value with such designations, preferences and participating, optional or other special rights and qualifications, limitations or restrictions thereof as shall be determined by the Company’s Board of Directors.
On May 1, 2013, the Company filed an amendment to its Articles of Incorporation and effected a 20-for-1 reverse stock split of its issued and outstanding shares of common stock, $0.001 par value, whereby 43,182,599 outstanding shares of the Company’s common stock were exchanged for 2,159,159 shares of the Company's common stock. All per share amounts and number of shares in the consolidated financial statements and related notes have been retroactively restated to reflect the reverse stock split resulting in the transfer of $41,024 from common stock to additional paid in capital at December 31, 2012.
NOTE 10 – SHARE BASED COMPENSATION
2012 Incentive Stock Option Plan
On February 12, 2012, the Company’s board of directors (“Board of Directors”) approved the 2012 Incentive Stock Option Plan (the “2012 Plan”). The 2012 Plan provides for the issuance of options to purchase up to 200,000 shares of the Company’s common stock to officers, directors, employees and consultants of the Company. Under the terms of the 2012 Plan, the Company may issue Incentive Stock Options as defined by the Internal Revenue Code to employees of the Company and may also issue nonstatutory options to employees and others. The Board of Directors of the Company determines the exercise price, vesting and expiration period of the grants under the 2012 Plan. However, the exercise price of an Incentive Stock Option may not be less than 110% of fair value of the common stock at the date of the grant for a 10% or more shareholder and 100% of fair value for a grantee who is not a 10% shareholder. The fair value of the common stock is determined based on quoted market price or in absence of such quoted market price, by the Board of Directors in good faith. Additionally, the vesting period of the grants under the 2012 Plan may not be more than five years and expiration period not more than ten years. The Company reserved 200,000 shares of its common stock for future issuance under the terms of the 2012 Plan.
On May 9, 2012, 175,000 options had been granted under the 2012 Plan. Of such options, 25,000 were cancelled and 150,000 were outstanding at December 31, 2013 with an exercise price of $30.00, a 10 year life and fair value of $23.50. The options vest 1/3rd on May 9, 2013 and 1/36th on the 9th of each month thereafter for 24 months.
On February 12, 2013, the 2012 Plan was amended and restated to increase the number of shares reserved under the plan to 550,000. On February 12, 2013, 226,500 options were granted under the 2012 Plan (all of which were outstanding at December 31, 2013) with an exercise price of $10.20, a 10 year life and fair value of $7.83. The options vest 1/3rd on February 12, 2014 and 1/36th on the 12th of each month thereafter for 24 months.
The Company measures the fair value of stock options on the date of grant, based on a Binomial option pricing model using certain assumptions discussed in the following paragraph, and the closing market price of the Company's common stock on the date of the grant. Stock options granted vest over a three year period and expire ten years from the date of grant. Share-based compensation expense related to awards is amortized over the applicable vesting period using the straight-line method.
The assumptions used in the valuation of stock options granted during the years ended December 31, 2013 and 2012 were as follows:
|
|
|
2012
|
|
|
2013
|
|
|
Risk-free interest rate
|
|
|
1.87
|
%
|
|
|
2.02
|
%
|
|
Expected term of option
|
|
|
6.5 years
|
|
|
|
6.0 years
|
|
|
Expected stock price volatility
|
|
|
95.89
|
%
|
|
|
99.96
|
%
|
|
Expected dividend yield
|
|
$
|
0.0
|
|
|
$
|
0.0
|
|
The risk-free interest rate is based on the yield of Daily U.S. Treasury Yield Curve Rates with terms equal to the expected term of the options as of the grant date. The expected term of options is determined using the simplified method, as provided in an SEC Staff Accounting Bulletin, and the expected stock price volatility is based on comparable companies’ historical stock price volatility since the Company does not have sufficient historical exercise or volatility data because its equity shares have been publicly traded for only a limited period of time.
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
Share-based compensation expense of $1,717,037 and $865,158 was recognized for the years ended December 31, 2013 and 2012, respectively.
As of December 31, 2013, the Company had approximately $2,798,281 of total unrecognized compensation cost related to non-vested awards granted under the Company’s 2012 option plan, which the Company expects to recognize over a weighted average period of 1.69 years.
A summary of the stock option activity and related information for the 2012 Plan for the years ended December 31, 2013 and 2012 is as follows:
|
|
Shares
|
|
Weighted-Average
Exercise Price
|
|
Weighted-Average
Remaining
Contractual Term
|
|
Aggregate Intrinsic
Value
|
|
|
Outstanding at January 1, 2012
|
|
|
-
|
|
|
|
|
|
|
|
|
|
|
|
Grants
|
|
|
175,000
|
|
$
|
30.00
|
|
|
10.00
|
|
$
|
-
|
|
|
Exercised
|
|
|
-
|
|
|
|
|
|
|
|
|
|
|
|
Forfeitures or expirations
|
|
|
(25,000)
|
|
$
|
30.00
|
|
|
|
|
|
|
|
|
Outstanding at January 1, 2013
|
|
|
150,000
|
|
$
|
30.00
|
|
|
9.35
|
|
$
|
-
|
|
|
Grants
|
|
|
226,500
|
|
$
|
10.20
|
|
|
10.00
|
|
$
|
-
|
|
|
Exercised
|
|
|
-
|
|
|
|
|
|
|
|
|
|
|
|
Forfeitures or expirations
|
|
|
-
|
|
|
|
|
|
|
|
|
|
|
|
Outstanding at December 31,
2013
|
|
|
376,500
|
|
$
|
18.09
|
|
|
8.81
|
|
$
|
24,915
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vested and expected to vest at
December 31, 2013
|
|
|
376,500
|
|
$
|
18.09
|
|
|
8.81
|
|
$
|
24,915
|
|
|
Exercisable at December 31,
2013
|
|
|
79,167
|
|
$
|
30.00
|
|
|
8.36
|
|
$
|
-
|
|
The aggregate intrinsic value in the preceding tables represents the total pretax intrinsic value, based on options with an exercise price less than the Company’s closing stock price of $10.31 as of December 31, 2013, which would have been received by the option holders had those option holders exercised their options as of that date.
NOTE 11 – STOCK WARRANTS
The following table summarizes information with respect to outstanding warrants to purchase common stock of the Company, all of which were exercisable, at December 31, 2013:
|
Exercise
|
|
|
Number
|
|
|
Expiration
|
|
|
Price
|
|
|
Outstanding
|
|
|
Date
|
|
|
$
|
4.25
|
|
|
2,312,130
|
|
|
August 2018
|
|
|
$
|
12.00
|
|
|
456,009
|
|
|
December 2017 to February 2018
|
|
|
$
|
20.00
|
|
|
15,288
|
|
|
January 2014 to January 2015
|
|
|
$
|
25.00
|
|
|
354,229
|
|
|
January 2017 to February 2019
|
|
|
|
|
|
|
3,137,656
|
|
|
|
|
On January 20, 2012, the Company issued an aggregate of 13,750 and 1,538 warrants to purchase the Company's common stock at an exercise price of $20.00 per share to convertible debenture holders and debenture placement agents, respectively (see Note 6). The warrants issued to convertible debenture holders expire three years from the date of issuance. Of the warrants issued to debenture placement agents, 750 expire two years from the date of issuance, and 788 expire three years from the date of issuance.
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
In connection with the January and March 2012 Financing, the Company issued to investors an aggregate of 215,148 and 115,741 warrants, respectively, to purchase the Company's common stock at an exercise price of $25.00 per share expiring five years from the date of issuance. In addition, the Company issued an aggregate of 11,765 and 11,575 warrants to purchase the Company's common stock at an exercise price of $25.00 per share expiring seven years from the date of issuance to placement agents. These warrants contained certain anti-dilutive provisions and were covered under a registration rights agreement (see Note 6).
In connection with the December 2012 Financing, the Company issued to investors 445,209 Class A warrants to purchase the Company's common stock. The Class A warrant is exercisable at $12.00 per share expiring five years from the date of issuance and may be exercised on a cashless basis under certain circumstances. These warrants are covered under a registration rights agreement (see Note 8).
On January 1, 2013, the Company issued warrants to non-employees to purchase 10,800 shares of the Company's common stock at an exercise price of $12.00 per share expiring five years from the date of issuance vesting ratably over twelve months beginning January 1, 2013 in connection with services.
In connection with the August 2013 Financing, the Company issued to investors warrants to purchase 2,680,000 shares of the Company's common stock. The warrants are exercisable at $4.25 per share, expire five years from the date of issuance, and may be exercised on a cashless basis under certain circumstances. In addition, the Company issued to the Underwriters warrants to purchase 509,200 shares of the Company's common stock. The warrants are exercisable at $4.25 per share, expire five years from the date of issuance, and may be exercised on a cashless basis.
The Company measures the fair value of the vested portion of the issued warrants based on a Binomial option pricing model using certain assumptions discussed in the following paragraph, and the closing market price of the Company's common stock on the date of the fair value determination.
The assumptions used in the valuation of warrants, which vested during the year ended December 31, 2013, were as follows:
|
Risk-free interest rate
|
|
|
0.77 to 1.75
|
%
|
|
Life of warrant
|
|
|
4.75 to 4.01 years
|
|
|
Expected stock price volatility
|
|
|
91.31% to 102.46
|
%
|
|
Expected dividend yield
|
|
$
|
0.0
|
|
The risk-free interest rate is based on the yield of Daily U.S. Treasury Yield Curve Rates with terms equal to the life of the warrants as of the grant date. The expected stock price volatility is based on comparable companies’ historical stock price volatility since the Company does not have sufficient historical volatility data because its equity shares have been publicly traded for only a limited period of time.
Compensation of $51,114 related to vested warrants was recognized for the year ended December 31, 2013.
As of December 31, 2013, there was no unrecognized compensation related to unvested warrants.
In April 2013, the Company issued an aggregate of 38,334 shares of its common stock upon the exercise of warrants at $8.00 per share.
In December 2013, the Company issued an aggregate of 873,885 and 70,031 shares of its common stock upon the exercise of warrants at $4.25 and $8.00 per share, respectively.
In December 2013, the Company issued 1,672 shares of its common stock upon the exercise of 3,185 warrants exercisable at $4.25 per share on a cashless basis.
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 12 – COMMITMENTS
Operating leases
On September 28, 2010, the Company entered into a five-year lease for office space in New York City, with monthly payments escalating from approximately $10,000 in the first year to approximately $11,000 in the fifth year. The Company received a rent credit of $9,420 in each of the months of November 2010, December 2010 and January 2011. The Company has posted a letter of credit in the amount of approximately $60,000 for the benefit of the landlord which is collateralized by a money market account (see Note 4 ).
Future minimum lease payments under the operating lease are as follows:
|
Year Ending December 31,
|
|
|
|
|
|
2014
|
|
$
|
131,513
|
|
|
2015
|
|
|
100,719
|
|
|
|
|
$
|
232,232
|
|
See note 15.
Rent expense charged to operations, which differs from rent paid due to the rent credits and to increasing amounts of base rent, is calculated by allocating total rental payments on a straight-line basis over the term of the lease. During the years ended December 31, 2013 and 2012, rent expense was $116,569 and $116,732, respectively and as of December 31, 2013 and 2012 deferred rent payable was $19,710 and $26,156, respectively, including the current portion included in accrued expenses.
Consulting agreements
During 2012 and 2013, the Company entered into contracts with various contract research organizations for which there are outstanding commitments aggregating approximately $4,500,000 at December 31, 2013 for future work to be performed.
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
NOTE 13 – INCOME TAXES
There is no provision for federal or state income taxes for the years ended December 31, 2013 and 2012 since the Company has established a valuation allowance equal to the total deferred tax asset related to losses incurred during such periods.
Deferred tax assets and liabilities and related valuation allowance as of December 31, 2013 and 2012 are as follows:
|
|
|
December 31,
|
|
|
|
|
2013
|
|
2012
|
|
|
Deferred tax assets:
|
|
|
|
|
|
|
|
|
Research and development credit carryforward (1)
|
|
|
6,188
|
|
|
6,188
|
|
|
Net operating loss carryforwards
|
|
|
9,040,045
|
|
|
5,207,759
|
|
|
Other
|
|
|
383,053
|
|
|
147,003
|
|
|
|
|
|
|
|
|
|
|
|
Total deferred tax assets
|
|
|
9,429,286
|
|
|
5,360,950
|
|
|
|
|
|
|
|
|
|
|
|
Valuation allowance
|
|
|
(9,429,286)
|
|
|
(5,360,950)
|
|
|
|
|
|
|
|
|
|
|
|
Net deferred tax assets
|
|
$
|
0
|
|
$
|
0
|
|
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
|
|
(1)
|
The Company has incurred research and development (“R&D”) expenses, a portion of which may qualify for tax credits. The Company has not conducted an R&D credit study to quantify the amount of credits and has not claimed an R&D credit on its federal tax returns filed except for $6,188 in 2007. The Company may conduct the study in future years and may establish the R&D credit carryforward for prior years. In such event, the net operating loss carryforward will be correspondingly reduced by the amount of the credit.
|
Based on the Company's historical losses and its expectation of continuation of losses for the foreseeable future, the Company has determined that it is not more likely than not that the deferred tax assets will be realized and accordingly, has provided a valuation allowance. The increase in the valuation allowance for the years ended December 31, 2013 and 2012 was $4,068,336 and $2,891,718, respectively.
At December 31, 2013, the Company has available unused net operating loss carryforwards of approximately $20.8 million that expire from 2027 to 2033 for federal tax purposes and $14.8 million for New Jersey state tax purposes, which expire from 2014 to 2033. The Company also has approximately $20.6 million of net operating loss carryforwards for New York State and New York City purposes expiring from 2030 to 2033. At December 31, 2013, the Company has a research and development carryforward of $6,188 for federal tax purposes that expires in 2027. These net operating loss and research and development credit carryforwards may be subject to annual limitations in their use in accordance with IRC Section 382. Accordingly, the extent to which such carryforwards can be used to offset future taxable income may be limited.
The Company's federal and state tax returns remain open and subject to examination by the tax authorities for the tax years 2010 and after.
A reconciliation of the effect of applying the federal statutory rate to the net loss and the effective income tax rate used to calculate the Company's income tax provision is as follows:
|
|
|
Year Ended
December 31,
|
|
|
|
|
2013
|
|
2012
|
|
|
Statutory federal income tax
|
|
(34.0)
|
%
|
(34.0)
|
%
|
|
State income tax, net of federal tax effect
|
|
(10.5)
|
%
|
(5.9)
|
%
|
|
Permanent difference
|
|
6.7
|
%
|
5.0
|
%
|
|
Increase in valuation allowance
|
|
37.8
|
%
|
34.9
|
%
|
|
|
|
|
|
|
|
|
Income tax provision
|
|
0
|
%
|
0
|
%
|
NOTE 14 – RELATED PARTY TRANSACTIONS
Dr. Seth Lederman, our Chief Executive Officer and Chairman of the Board, and Dr. Donald Landry, one of our directors, are the primary founders of the Company. We have entered into various transactions with several companies under their control, including L&L, Plumbline, Targent Pharmaceuticals, LLC and Lederman & Co. Total expenses paid under these agreements were $271,875 and $300,583 during the years ended December 31, 2013 and 2012, respectively.
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
On November 14, 2012, the Company sold to officers, members of the board of directors and their related parties for aggregate cash proceeds of $390,000, debentures (the “Debentures”) in the principal face amount of $390,000 and exchanged Debentures in the principal face amount of $320,000 for promissory notes issued between October and November 2012 to some affiliated investors. In December 2012, the Debentures were exchanged for the December 2012 Units at a conversion price of $6.00 per share. Interest expense on the Debentures for the year ended December 31, 2012 was $3,155 (see Note 7).
On July 31, 2013, the Company sold two promissory notes in the principal face amounts of $150,000 and $50,000 to Lederman & Co and Eli Lederman, respectively, and on August 1, 2013, the Company sold a promissory note in the principal face amount of $80,000 to Lederman & Co. The notes, which were sold for an aggregate of $280,000, are payable on demand at any time after one year from issuance and bear no interest.
NOTE 15 – SUBSEQUENT EVENTS
Commitments
Between January 1, 2014 and March 27, 2014, the Company entered into contracts with various contract research organizations for which there are outstanding commitments aggregating approximately $5,600,000 for future work to be performed.
On February 11, 2014, the Company entered into a lease amendment and expansion agreement, whereby the Company agreed to lease additional premises for office space, commencing May 1, 2014 and expiring on April 30, 2019. An increase to the original letter of credit will be required in the amount of $72,354. Future minimum lease payments under the agreement are as follows:
|
Year Ending December 31,
|
|
|
|
|
|
2014
|
|
$
|
220,085
|
|
|
2015
|
|
$
|
269,844
|
|
|
2016
|
|
$
|
277,509
|
|
|
2017
|
|
$
|
285,404
|
|
|
2018
|
|
$
|
293,537
|
|
|
2019
|
|
$
|
98,758
|
|
Related Party Transactions
On March 18, 2014, Tonix Barbados entered into an agreement with Leder Laboratories, Inc. (“Leder”), to acquire intellectual property related to novel smallpox vaccines. As consideration, $125,000 in cash and 25,000 shares of the Company’s common stock were paid to Leder.
On March 18, 2014, Tonix Barbados entered into an agreement with Starling Pharmaceuticals, Inc. (“Starling”), to acquire intellectual property related to radio and chemo protective agents. As consideration, $125,000 in cash and 25,000 shares of the Company’s common stock were paid to Starling.
Leder and Starling are wholly-owned entities in which Dr. Seth Lederman, the Chief Executive Officer and Chairman of the Board of the Company, has a controlling interest.
Equity transactions
From January 1 through March 27, 2014, the Company issued an aggregate of 1,127,866 shares of its common stock upon the exercise of warrants at $4.25 per share. Net proceeds received was approximately $4,800,000. On January 24, 2014, the Company entered into an underwriting agreement with Roth Capital Partners, LLC, as representative of several underwriters, relating to the issuance and sale of 2,898,550 shares of the Company’s common stock at a public offering price of $15.00 per share.
On January 29, 2014, the Company sold the shares for net proceeds of approximately $40.7 million, after deducting underwriting discounts and commissions and other offering expenses.
TONIX PHARMACEUTICALS HOLDING CORP.
(a development stage company)
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2013 AND 2012
Options granted
On February 11, 2014, the Company granted options to purchase an aggregate of 173,500 shares of the Company’s common stock to officers and key employees at an exercise price equal to the volume weighted average price of the Company stock 30 calendar days prior to February 11, 2014 for a period of ten years, vesting 1/3 on the first anniversary and 1/36th each month thereafter for 24 months.
Lederman Employment Agreement
On February 11, 2014, the Company entered into an employment agreement (the “Agreement”) with Dr. Seth Lederman (“Lederman”) to continue to serve as our President, Chief Executive Officer and Chairman of the board of directors of the Company (the “Board”). Previously, the Company entered into a consulting agreement with Lederman & Co., LLC, pursuant to which Lederman received compensation for serving as the Company’s President and Chief Executive Officer. On February 11, 2014, the consulting agreement was terminated.
The Agreement provides for various payment and benefits to Lederman in the event Lederman’s employment is terminated without cause (as defined) or Lederman resigns for Good Reason (as defined) as well as in the event employment is terminated as a result of death or permanent disability.
Defined Contribution Plan
Effective March 3, 2014, the Company established a qualified defined contribution plan (the “401(k) Plan”) pursuant to Section 401(k) of the Internal Revenue Code of 1986, as amended (the “Code”), whereby all eligible employees may participate. Participants may elect to defer a percentage of their annual pretax compensation to the 401(k) plan, subject to defined limitations. The Company is required to make contributions to the 401(k) Plan equal to 100 percent of each participant’s pretax contributions of up to 19 percent of his or her eligible compensation, and the Company is also required to make a contribution equal to 6 percent of each participant’s salary, on an annual basis, subject to limitations under the Code.
ITEM 9 - CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURES
None.
ITEM 9A – CONTROLS AND PROCEDURES
(a) Evaluation of disclosure controls and procedures.
Our management, with the participation of our Chief Executive Officer and Chief Financial Officer, evaluated the effectiveness of our disclosure controls and procedures pursuant to Rule 13a-15 under the Exchange Act. In designing and evaluating the disclosure controls and procedures, management recognizes that any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving the desired control objectives. In addition, the design of disclosure controls and procedures must reflect the fact that there are resource constraints and that management is required to apply its judgment in evaluating the benefits of possible controls and procedures relative to their costs.
Based on management’s evaluation, our Chief Executive Officer and Chief Financial Officer concluded that our disclosure controls and procedures are designed at a reasonable assurance level and are effective to provide reasonable assurance that information we are required to disclose in reports that we file or submit under the Exchange Act is recorded, processed, summarized, and reported within the time periods specified in SEC rules and forms, and that such information is accumulated and communicated to our management, including our chief executive officer and chief financial officer, as appropriate, to allow timely decisions regarding required disclosure.
(b) Changes in internal control over financial reporting.
There were no changes in our internal control over financial reporting that occurred during the quarter ended December 31, 2013 that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
(c) Management’s report on internal control over financial reporting.
Our management is responsible for establishing and maintaining adequate internal control over financial reporting, as defined in Exchange Act Rule 13a-15(f). Management conducted an evaluation of the effectiveness of our internal control over financial reporting based on the framework in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission. Based on this evaluation, management concluded that our internal control over financial reporting was effective as of December 31, 2012.
This annual report does not include an attestation report by EisnerAmper LLP, our independent registered public accounting firm regarding internal control over financial reporting. As a smaller reporting company, our management's report was not subject to attestation by our registered public accounting firm pursuant to rules of the Securities and Exchange Commission that permit us to provide only management's report in this annual report.
ITEM 9B – OTHER INFORMATION
None.
PART III
ITEM 10 – DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE
The names of our executive officers and directors and their age, title, and biography as of March 24, 2014 are set forth below:
|
Name
|
|
Age
|
|
Title
|
|
Seth Lederman
|
|
56
|
|
President, CEO and Chairman of the Board of Directors
|
|
Leland Gershell
|
|
41
|
|
Chief Financial Officer and Treasurer
|
|
Bruce Daugherty
|
|
56
|
|
Chief Scientific Officer, Controller and Secretary
|
|
Stuart Davidson
|
|
56
|
|
Director
|
|
Patrick Grace
|
|
57
|
|
Director
|
|
Donald W. Landry
|
|
59
|
|
Director
|
|
Ernest Mario
|
|
75
|
|
Director
|
|
Charles E. Mather IV
|
|
53
|
|
Director
|
|
John Rhodes
|
|
57
|
|
Lead Director
|
|
Samuel Saks
|
|
59
|
|
Director
|
Directors are elected annually and hold office until the next annual meeting of the stockholders of the Company and until their successors are elected. Officers are elected annually and serve at the discretion of the Board of Directors.
Seth Lederman, MD became our President, Chief Executive Officer, Chairman of the Board and a Director in October 2011. Dr. Lederman founded Tonix Sub in June of 2007 and has acted as its Chairman of the Board of Directors since inception and as President since June 2010. Dr. Lederman has been the Chairman of Krele since its inception in August 2010. Dr. Lederman has also been the President and a director of Tonix Pharmaceuticals (Canada), Inc. since its inception in April 2013. Since 1996, Dr. Lederman has been an Associate Professor at Columbia University. As an Assistant Professor at Columbia, Dr. Lederman discovered and characterized the CD40-ligand and invented therapeutic candidates to treat autoimmune diseases and transplant rejection. Dr. Lederman has been a Manager of L&L since 1996. In addition, Dr. Lederman has been the Managing Member of Seth Lederman Co, LLC since January 2007 and the Managing Member of Lederman & Co since 2002, both of which are biopharmaceutical consulting and investing companies. Dr. Lederman has also been the Managing Member of Targent since 2000, and Managing Member of Plumbline since 2002. Targent was a founder of Targent Pharmaceuticals Inc. on which Board of Directors Dr. Lederman served from inception in 2001 until the sale of its assets to Spectrum Pharmaceuticals Inc. in 2006. Between January 2007 and November 2008, Dr. Lederman was a Managing Partner of Konanda Pharma Partners, LLC, a Director of Konanda Pharma Fund I, LP, and a Managing Partner of Konanda General Partner, LLC, which were related private growth equity fund entities. As well, between January 2007 and November 2008, Dr. Lederman was Chairman of Validus Pharmaceuticals, Inc. and Fontus Pharmaceuticals, Inc., which were portfolio companies of the Konanda private growth equity fund. Since December 2011, Dr. Lederman has served as CEO and Chairman of Leder Laboratories Inc. and Starling Pharmaceuticals Inc, which are biopharmaceutical development companies. Since March 2013, Dr. Lederman has been the chairman of Leder Laboratories, Ltd., a wholly-owned subsidiary of Leder Laboratories Inc. Between 2006 and 2011, Dr. Lederman was a director of Research Corporation, a New York-based non-profit organization. Dr. Lederman received his BA degree in Chemistry from Princeton University in 1979 and his MD from Columbia University in 1983. Dr. Lederman has been a New York State licensed physician since 1985. Dr. Lederman’s significant experience with our patent portfolio and his experience as an entrepreneur, seed capital investor, fund manager, and director of start-up biopharmaceutical companies were instrumental in his selection as a member of the board of directors.
Leland Gershell, MD PhD became our Chief Financial Officer in April 2012 and our Treasurer in November 2012. From May 2011 to December 2011, Dr. Gershell was Managing Director and Senior Analyst at Madison Williams and Company, where he was responsible for equity research coverage of specialty pharmaceutical and biotechnology companies. From April 2010 to October 2010, Dr. Gershell was Senior Analyst at Favus Institutional Research, where he was responsible for issuing research reports on a variety of healthcare companies to institutional investors. From October 2008 to October 2009, Dr. Gershell was Senior Analyst at Apothecary Capital, a healthcare investment firm. From November 2004 to September 2008, Dr. Gershell was an equity research analyst at Cowen and Company, most recently as Vice President, where he was responsible for the equity research coverage of small and middle capitalization biotechnology companies. Dr. Gershell earned his M.D. and Ph.D. in Organic Chemistry from Columbia University and his B.A. magna cum laude in Chemistry and Asian Studies from Dartmouth College. Dr. Gershell is an inventor on patents for SAHA/vorinostat, which is marketed by Merck as Zolinza® and is the first histone deacetylase (HDAC) inhibitor to receive FDA approval.
Bruce Daugherty, PhD became our Controller in April 2012, our Secretary in November 2012 and our Chief Scientific Officer in August 2013. Between April 2012 and August 2013, Dr. Daugherty was our Senior Director of Drug Development. Dr. Daugherty has also been the Secretary and a director of Tonix Pharmaceuticals (Canada), Inc. since its inception in April 2013. Since January 2009, Dr. Daugherty has worked as a consultant to academia and biotechnology companies in drug discovery/development and licensing through his consulting company, LeClair Pharma Consulting, LLC. Dr. Daugherty was a consultant to our company between November 2011 and March 2012. In 2009, Dr. Daugherty was employed at Assumption College in Mendham, New Jersey, where he was a lecturer in Biology for freshman students. From 1987 to 2008, Dr. Daugherty was employed at Merck & Co., where he was a scientist in drug discovery and development. Dr. Daugherty earned his MBA from Emory University’s Goizueta Business School, his PhD in Molecular Genetics and Microbiology from Rutgers University-Robert Wood Johnson Medical School, his MS in Zoology from Rutgers University and his BA in Biology from Washington University in St. Louis.
Stuart Davidson became a Director in October 2011. Between July 2010 and October 2011, Mr. Davidson served as a director of Tonix Sub. Since 2011, Mr. Davidson has been a Managing Director of Sonen Capital. Since 1994, Mr. Davidson has been a Managing Partner of Labrador Ventures. Prior to Labrador, Mr. Davidson founded and served as CEO of Combion, Inc., which was acquired by Incyte. He also served as President of Alkermes, Inc., a biotechnology company focused on drug delivery. Mr. Davidson received his Bachelor’s Degree from Harvard College in 1978 and his MBA from Harvard Business School in 1984. Mr. Davidson’s prior experience as a venture capital investor, entrepreneur, and biotechnology industry executive experience leading pharmaceutical companies was instrumental in his selection as a member of our board of directors.
Patrick Grace became a Director in October 2011. Between June 2007 and October 2011, Mr. Grace served as a director of Tonix Sub. Mr. Grace was the co-founder of and served as the Managing Partner of Apollo Philanthropy Partners, L.L.C. from October 2008 until October 2012. He has also been President of MLP Capital, Inc., New York, New York, an investment holding company, since 1996. Mr. Grace served in various senior management roles with W. R. Grace & Co. from 1977 – 1995, and was last President and CEO of Grace Logistics Services, Inc. From January 2002 to August 2002, Mr. Grace was also President and Chief Executive Officer of Kingdom Group, LLC (“Kingdom”), New York, New York (a provider of turnkey compressed natural gas fueling systems), and he was Executive Vice President of Kingdom from August 1999 to December 2000. Since 1996, he has been a director of Chemed Corporation. Mr. Grace was a liberal arts major at the University of Notre Dame and earned a MBA in finance from Columbia University. Mr. Grace’s extensive executive experience, along with his membership on the board of directors of a public company was instrumental in his selection as a member of our board of directors.
Donald W. Landry, MD, PhD became a Director in October 2011. Between June 2007 and October 2011, Dr. Landry served as a director of Tonix Sub. Dr. Landry has been a member of the faculty of Columbia University since 1986, and has served as the Samuel Bard Professor of Medicine, Chair of the Department of Medicine and Physician-in-Chief at New York Presbyterian Hospital/Columbia University since 2008. Dr. Landry was a co-founder and has been a member of L&L since 1996. Dr. Landry received his BS degree in Chemistry from Lafayette College in 1975, his PhD in Organic Chemistry from Harvard University in 1979 and his M.D. from Columbia University in 1983. Dr. Landry has been a New York State licensed physician since 1985. In 2008, Dr. Landry was awarded the Presidential Citizens Medal, the second-highest award that the President can confer upon a civilian. Dr. Landry’s significant medical and scientific background was instrumental in his selection as a member of the board of directors.
Ernest Mario, PhD became a Director in October 2011. Between September 2010 and October 2011, Dr. Mario served as a director of Tonix Sub. Dr. Mario is a former Deputy Chairman and Chief Executive of Glaxo Holdings plc and a former Chairman and Chief Executive Officer of ALZA Corporation. Since February 2014, Dr. Mario has served as Executive Chairman of Capnia, Inc., a privately held specialty pharmaceutical company in Palo Alto, CA. Between August 2007 and February 2014, Dr. Mario served as the Chief Executive Officer and Chairman of Capnia, Inc. From 2003 to 2007, he was Chairman and Chief Executive of Reliant Pharmaceuticals, Inc. Dr. Mario is currently a Director of Boston Scientific Corp. (since 2001), Celgene Corp. (since 2007), Chimerix, Inc. (since February 2013), Kindred Biosciences, Inc. (since February 2013) and XenoPort Inc. (since 2012). Dr. Mario is also Chairman of Chimerix. He is Chairman of the American Foundation for Pharmaceutical Education and serves as an advisor to The Ernest Mario School of Pharmacy at Rutgers University. In 2007, Dr. Mario was awarded the Remington Medal by the American Pharmacists’ Association, pharmacy’s highest honor. Dr. Mario received a PhD and an MS in physical sciences from the University of Rhode Island and a BS in pharmacy from Rutgers University. Dr. Mario brings to his service as a director his significant executive leadership experience, including his experience leading several pharmaceutical companies, as well as his membership on public company boards and foundations. He also has extensive experience in financial and operations management, risk oversight, and quality and business strategy.
Charles E. Mather IV became a Director in October 2011. Between April and October 2011, Mr. Mather served as a director of Tonix Sub. Mr. Mather has been the Head of Private and Alternative Capital and Co-Head of ECM at Janney Montgomery Scott since December 2009. Between October 2008 and December 2009, Mr. Mather served as an independent consultant to various securities firms. Between May 2007 and September 2008, Mr. Mather was the head of the Structured Equity Group at Jefferies Group Inc. Prior to that, Mr. Mather held various senior investment banking positions at Cowen and Company, including as Co-Head of the Private Equity Group. Mr. Mather received a BA in History from Brown University and an MBA in Finance from The Wharton School, University of Pennsylvania. Mr. Mather’s extensive experience as an investment banker was instrumental in his selection as a member of our board of directors.
John Rhodes became a Director in October 2011 and Lead Director in February 2014. Mr. Rhodes has served as President and CEO of the New York State Energy Research and Development Authority since September 2103. Between October 2010 and October 2011, Mr. Rhodes served as a director of Tonix Sub. Mr. Rhodes has been a director of Dewey Electronics Company, a manufacturer of electronic and electromechanical systems for the military and commercial markets, since 2005, until 2013. Between January 2013 and September 2103, he served as director of the Center for Market Innovation at Natural Resources Defense Council. Between April 2007 and June 2010, Mr. Rhodes was a Senior Advisor to Good Energies, Inc., a renewable energy company. Mr. Rhodes is a former Vice President of Booz Allen Hamilton, Inc. Mr. Rhodes is a graduate of Princeton University and the Yale School of Management. Mr. Rhodes’ extensive business and consulting experience, along with his membership on the board of directors of a public company was instrumental in his selection as a member of our board of directors.
Samuel Saks, MD became a Director in May 2012. Between 2003 and April 2009, Dr. Saks was the chief executive officer and a director of Jazz Pharmaceuticals, Inc., a publicly-held biopharmaceutical company, which he co-founded in 2003. From April 2011 until February 2012, Dr. Saks served as interim Chief Medical Officer of Threshold Pharmaceuticals, a publicly-held biopharmaceutical company. From 2001 until 2003, Dr. Saks was company group chairman of ALZA Corporation and a member of the Johnson & Johnson Pharmaceuticals Operating Committee. From 1992 until 2001, Dr. Saks held various positions at ALZA, including Chief Medical Officer and Group Vice President, where he was responsible for clinical, regulatory and commercial activities. Previously, Dr. Saks held clinical research and development management positions with Schering-Plough, Xoma and Genentech. Dr. Saks formerly served as a scientific advisor to ArQule Pharmaceuticals, CMEA Ventures and ProQuest Investments. Dr. Saks is currently a Director of Auspex Pharmaceuticals, Inc. (since 2009), Depomed (since 2012), Bullet Biotechnology, Inc. (since 2012), Velocity Pharmaceutical Development LLC (since 2011) and NuMedii (since 2013). From September 2005 until October 2010, Dr. Saks served on the board of directors of Trubion Pharmaceuticals, a publicly-held biopharmaceutical company. Between September 2007 and July 2009, Dr. Saks served on the board of directors of Cougar Biotechnology, a publicly-held biopharmaceutical company. Dr. Saks has also served on the board of directors of Corixa, Coulter and Ribozyme. Dr. Saks is board certified in oncology and received a B.S. and an M.D. from the University of Illinois. Mr. Saks’ extensive scientific and medical expertise and experience in formulating partnering and business development strategies, including those involving larger pharmaceutical companies, was instrumental in his selection as a member of our board of directors.
Family Relationships
None.
Board Independence
We are not required to have any independent members of the Board of Directors. The board of directors has determined that (i) Seth Lederman, has a relationship which, in the opinion of the board of directors, would interfere with the exercise of independent judgment in carrying out the responsibilities of a director and is not an “independent director” as defined in the Marketplace Rules of The NASDAQ Stock Market and (ii) Stuart Davidson, Patrick Grace, Donald Landry, Ernest Mario, Charles Mather, John Rhodes and Samuel Saks are each an independent director as defined in the Marketplace Rules of The NASDAQ Stock Market.
Meetings and Committees of the Board of Directors
During the fiscal year ended December 31, 2013, our board of directors held four meetings and approved certain actions by unanimous written consent. We expect our directors to attend all board and committee meetings and to spend the time needed and meet as frequently as necessary to properly discharge their responsibilities.
Audit Committee
Our Audit Committee consists of Patrick Grace, Charles Mather and John Rhodes, with Mr. Grace elected as Chairman of the Committee. Our Board of Directors has determined that each of Messrs. Grace, Mather and Rhodes are “independent” as that term is defined under applicable SEC rules and under the current listing standards of the NASDAQ Stock Market. Mr. Grace is our audit committee financial expert.
Our Audit Committee’s responsibilities include: (i) reviewing the independence, qualifications, services, fees, and performance of the independent auditors, (ii) appointing, replacing and discharging the independent auditor, (iii) pre-approving the professional services provided by the independent auditor, (iv) reviewing the scope of the annual audit and reports and recommendations submitted by the independent auditor, and (v) reviewing our financial reporting and accounting policies, including any significant changes, with management and the independent auditor. The Audit Committee has reviewed and discussed with management the Company’s audited financial statements for the year ended December 31, 2012. Based on the reviews and discussions referred to above, the Audit Committee has recommended to the Board of Directors that the financial statements referred to above be included in this Form 10-K.
Compensation Committee
Our Compensation Committee consists of Stuart Davidson, Ernest Mario and Samuel Saks, with Mr. Davidson elected as Chairman of the Committee. Our Board of Directors has determined that all of the members are “independent” under the current listing standards of the NASDAQ Stock Market. Our Board of Directors has adopted a written charter setting forth the authority and responsibilities of the Compensation Committee.
Our Compensation Committee has responsibility for assisting the Board of Directors in, among other things, evaluating and making recommendations regarding the compensation of our executive officers and directors, assuring that the executive officers are compensated effectively in a manner consistent with our stated compensation strategy, producing an annual report on executive compensation in accordance with the rules and regulations promulgated by the SEC, periodically evaluating the terms and administration of our incentive plans and benefit programs and monitoring of compliance with the legal prohibition on loans to our directors and executive officers.
Governance and Nominating Committee
Our Governance and Nominating Committee consists of Donald Landry, Charles Mather and John Rhodes, with Mr. Rhodes elected as Chairman of the Committee. The Board of Directors has determined that all of the members are “independent” under the current listing standards of the NASDAQ Stock Market.
Our Governance and Nominating Committee has responsibility for assisting the Board in, among other things, effecting the organization, membership and function of the Board and its committees. The Governance and Nominating Committee shall identify and evaluate the qualifications of all candidates for nomination for election as directors. In addition, the Governance and Nominating Committee is responsible for developing, recommending and evaluating corporate governance standards and a code of business conduct and ethics.
Involvement in Certain Legal Proceedings
Our Directors and Executive Officers have not been involved in any of the following events during the past ten years:
|
|
1. |
any bankruptcy petition filed by or against such person or any business of which such person was a general partner or executive officer either at the time of the bankruptcy or within two years prior to that time; |
|
|
2. |
any conviction in a criminal proceeding or being subject to a pending criminal proceeding (excluding traffic violations and other minor offenses); |
|
|
3. |
being subject to any order, judgment, or decree, not subsequently reversed, suspended or vacated, of any court of competent jurisdiction, permanently or temporarily enjoining him from or otherwise limiting his involvement in any type of business, securities or banking activities or to be associated with any person practicing in banking or securities activities; |
|
|
4. |
being found by a court of competent jurisdiction in a civil action, the Securities and Exchange Commission or the Commodity Futures Trading Commission to have violated a federal or state securities or commodities law, and the judgment has not been reversed, suspended, or vacated; |
|
|
5. |
being subject of, or a party to, any federal or state judicial or administrative order, judgment decree, or finding, not subsequently reversed, suspended or vacated, relating to an alleged violation of any federal or state securities or commodities law or regulation, any law or regulation respecting financial institutions or insurance companies, or any law or regulation prohibiting mail or wire fraud or fraud in connection with any business entity; or |
|
|
6. |
being subject of or party to any sanction or order, not subsequently reversed, suspended, or vacated, of any self-regulatory organization, any registered entity or any equivalent exchange, association, entity or organization that has disciplinary authority over its members or persons associated with a member. |
Section 16(a) Beneficial Owner Reporting Compliance
Section 16(a) of the Securities Exchange Act of 1934, as amended, requires our directors, executive officers and holders of more than 10% of our common stock to file with the SEC reports regarding their ownership and changes in ownership of our securities We believe that, during fiscal 2013, our directors, executive officers and 10% stockholders complied with all Section 16(a) filing requirements.
Code of Ethics
We have adopted a Code of Ethics and Business Conduct that applies to all of our directors, officers and employees. A copy of the Code of Ethics is incorporated by reference as an exhibit.
ITEM 11 - EXECUTIVE COMPENSATION
Summary Compensation Table
The following table provides certain summary information concerning compensation awarded to, earned by or paid to our Chief Executive Officer, the two highest paid executive officers and up to two other highest paid individuals whose total annual salary and bonus exceeded $100,000 for fiscal years 2013 and 2012.
|
Name & Principal
Position
|
|
Year
|
|
Salary
($)
|
|
Bonus
($)
|
|
Stock
Awards
($)
|
|
Option
Awards
($)
|
|
Non-Equity
Incentive Plan
Compensation
($)
|
|
Change in
Pension Value
and
Non-Qualified
Deferred
Compensation
Earnings ($)
|
|
All Other
Compensation
($)
|
|
|
Total ($)
|
|
|
Seth Lederman (1)
|
|
2013
|
|
|
-
|
|
|
277,500
|
|
|
-
|
|
|
528,525
|
|
|
-
|
|
|
-
|
|
|
265,625
|
(2)
|
|
|
1,071,650
|
|
|
Chief Executive Officer
|
|
2012
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
822,715
|
|
|
-
|
|
|
-
|
|
|
279,750
|
(2)
|
|
|
1,102,465
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Leland Gershell (3)
|
|
2013
|
|
|
185,415
|
|
|
128,750
|
|
|
-
|
|
|
411,075
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
|
725,240
|
|
|
Chief Financial Officer
|
|
2012
|
|
|
138,542
|
|
|
-
|
|
|
-
|
|
|
587,654
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
|
726,196
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Bruce Daugherty (4)
|
|
2013
|
|
|
150,662
|
|
|
87,500
|
|
|
-
|
|
|
234,900
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
|
473,062
|
|
|
Chief Scientific Officer
|
|
2012
|
|
|
110,833
|
|
|
-
|
|
|
-
|
|
|
470,123
|
|
|
-
|
|
|
-
|
|
|
-
|
|
|
|
580,956
|
|
|
|
(1) |
Dr. Lederman became our President and Chief Executive Officer on October 7, 2011. His compensation reflects payments made to him either through Tonix or Tonix Sub. |
|
|
(2) |
Represents $0 and $40,000 of consulting fees paid to L&L, and $265,625 and $239,750 of consulting fees paid to Lederman & Co for the years ended December 31, 2013 and 2012, respectively. |
|
|
(3) |
Dr. Gershell became our Chief Financial Officer on April 1, 2012 and our Treasurer in November 2012. |
|
|
(4) |
Dr. Daugherty became our Senior Director of Drug Development and Controller on April 1, 2012. Dr. Daugherty became our Secretary in November 2012. Dr. Daugherty became our Chief Scientific Officer on August 14, 2013. |
Option/SAR Grants in Fiscal Year Ended December 31, 2013
|
Name
|
|
Grant Date
|
|
All Other Option Awards:
Number of Securities
Underlying Options (#)
|
|
Exercise or Base Price of
Option Awards ($/Share)
|
|
Grant Date Fair Value of
Stock and Option Awards
($)
|
|
|
Seth Lederman
|
|
2/12/2013
|
|
67,500
|
|
$
|
10.20
|
|
$
|
7.83
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Leland Gershell
|
|
2/12/2013
|
|
52,500
|
|
$
|
10.20
|
|
$
|
7.83
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Bruce Daugherty
|
|
2/12/2013
|
|
30,000
|
|
$
|
10.20
|
|
$
|
7.83
|
|
Outstanding Equity Awards at Fiscal Year-End Table
The following table sets forth information for the named executive officers regarding the number of shares subject to both exercisable and unexercisable stock options, as well as the exercise prices and expiration dates thereof, as of December 31, 2013.
|
Name
|
|
Number of
Securities
underlying
Unexercised
Options (#)
Exercisable
|
|
Number of
Securities
underlying
Unexercised
Options (#)
Unexercisable
|
|
Option
Exercise
Price ($/Sh)
|
|
Option Expiration Date
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Seth Lederman
|
|
18,471
|
|
16,529
|
|
$
|
30.00
|
|
5/9/2022
|
|
|
|
|
-
|
|
67,500
|
|
$
|
10.20
|
|
2/12/2023
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Leland Gershell
|
|
13,192
|
|
11,808
|
|
$
|
30.00
|
|
5/9/2022
|
|
|
|
|
-
|
|
52,500
|
|
$
|
10.20
|
|
2/12/2023
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Bruce Daugherty
|
|
10,559
|
|
9,441
|
|
$
|
30.00
|
|
5/9/2022
|
|
|
|
|
-
|
|
30,000
|
|
$
|
10.20
|
|
2/12/2023
|
|
Equity Compensation Plan Information
|
Plan category
|
|
|
Number of
securities to
be issued
upon
exercise of
outstanding
options
(a)
|
|
Weighted-
average
exercise
price of
outstanding
options
(b)
|
|
Securities remaining
available for future
issuance under equity
compensation plans
(excluding securities
reflected in column (a))
(c)
|
|
|
Equity compensation plans approved by security holders
|
|
|
376,500
|
|
$
|
18.09
|
|
173,500
|
|
|
Equity compensation plans not approved by security holders
|
|
|
-
|
|
|
-
|
|
-
|
|
|
Total
|
|
|
376,500
|
|
$
|
18.09
|
|
173,500
|
|
Employment Contracts and Termination of Employment and Change-In-Control Arrangements
Employment Agreements with Seth Lederman, Leland Gershell and Bruce Daugherty
On February 11, 2014, the Company entered into an employment agreement (the “Lederman Agreement”) with Dr. Seth Lederman (“Lederman”) to continue to serve as our President, Chief Executive Officer and Chairman of the board of directors of the Company (the “Board”). On March 14, 2014, the Company entered into an employment agreement (the “Daugherty Agreement”) with Dr. Bruce Daugherty (“Daugherty”) to continue to serve as our Chief Scientific Officer. On March 19, 2014, the Company entered into an employment agreement (the “Gershell Agreement” and together with the Lederman Agreement and Daugherty Agreement, the “Agreements”) with Dr. Leland Gershell (“Gershell” and together with Lederman and Daugherty, the “Executives”) to continue to serve as our Chief Financial Officer and Treasurer.
The base salaries for Lederman, Gershell and Daugherty under the Agreements are $425,000, $325,000 and $220,000 per annum, respectively. The Agreements have an initial term of one year and automatically renew for successive one year terms unless either party delivers written notice not to renew at least 60 days prior to the end of the current term.
Pursuant to the Agreements, if the Company terminates Executive’s employment without Cause (as defined in the Agreements) or Executive resigns for Good Reason (as defined in the Agreement), the Executive is entitled to the following payments and benefits: (1) his fully earned but unpaid base salary through the date of termination at the rate then in effect, plus all other benefits, if any, under any group retirement plan, nonqualified deferred compensation plan, equity award plan or agreement, health benefits plan or other group benefit plan to which Executive may be entitled to under the terms of such plans or agreements; (2) a lump sum cash payment in an amount equal to 12 months of his base salary as in effect immediately prior to the date of termination; (3) continuation of health benefits for Executive and his eligible dependents for a period of 12 months following the date of termination; and (4) the automatic acceleration of the vesting and exercisability of outstanding unvested stock awards as to the number of stock awards that would have vested over the 12-month period following termination had such Executive remained continuously employed by the Company during such period.
Pursuant to the Agreement, if Executive’s employment is terminated as a result of death or permanent disability, Executive or his estate, as applicable, is entitled to the following payments and benefits: (1) his fully earned but unpaid base salary through the end of the month in which termination occurs (except that for Lederman, it is through the date of termination) at the rate then in effect; (2) a lump sum cash payment in an amount equal to six months of his base salary as in effect immediately prior to the date of termination; and (3) the automatic acceleration of the vesting and exercisability of outstanding unvested stock awards.
If Executive is terminated without Cause or resigns for Good Reason during the period commencing 90 days prior to a Change in Control (as defined below) or 12 months following a Change in Control, Lederman shall be entitled to receive, in lieu of the severance benefits described above, the following payments and benefits: (1) a lump sum cash payment in an amount equal to 36 months (18 months for Gershell and Daugherty) of his base salary as in effect immediately prior to the date of termination, except that, while Executive is still entitled to the Sale Bonus (as defined below), it will only be 18 months (9 months for Gershell and Daugherty); (2) continuation of health benefits for Executive and his eligible dependents for a period of 24 months (12 months for Gershell and Daugherty) following the date of termination, except that, while Executive is still entitled to the Sale Bonus it will only be 12 months (6months for Gershell and Daugherty); and (3) the automatic acceleration of the vesting and exercisability of outstanding unvested stock awards.
If during the term of the Agreement or within 120 days after Executive is terminated without Cause or resigns for Good Reason, following a Change in Control, the Company consummates a Change in Control transaction in which the Enterprise Value (as defined below) equals or exceeds $50 million, Executive shall be entitled to receive a lump sum payment equal to (i) for Lederman, 4.4% of the Enterprise Value, (ii) for Gershell, 2.0% of the Enterprise Value, and (iii) for Daugherty, 1.6% of the Enterprise Value (the “Sale Bonus”). The Sale Bonus provision of the Agreement will terminate upon the Company granting Executive long-term incentive compensation mutually agreed to by the Board and such Executive.
For purposes of the Agreements, “Cause” generally means (1) commission of an act of fraud, embezzlement or dishonesty or some other illegal act that has a demonstrable material adverse impact on the Company or any successor or affiliate of the Company, (2) conviction of, or entry into a plea of “guilty” or “no contest” to, a felony, and (3) unauthorized use or disclosure of the Company’s confidential information or trade secrets or any successor or affiliate of the Company that has, or may reasonably be expected to have, a material adverse impact on any such entity.
For purposes of the Lederman Agreement, “Cause” also means (1) gross negligence, failure to follow a material, lawful and reasonable request of the Board or material violation of any duty of loyalty to the Company or any successor or affiliate of the Company, or any other demonstrable material willful misconduct by Lederman, (2) ongoing and repeated failure or refusal to perform or neglect of his duties as required by his employment agreement, which failure, refusal or neglect continues for 30 days following Lederman’s receipt of written notice from the Board stating with specificity the nature of such failure, refusal or neglect, provided that such failure to perform is not as a result of illness, injury or medical incapacity, or (3) material breach of any Company policy or any material provision of the Lederman Agreement.
For purposes of the Gershell Agreement and Daugherty Agreement, “Cause” also means (1) gross negligence, failure to follow a material, lawful and reasonable request of the CEO or material violation of any duty of loyalty to the Company or any successor or affiliate of the Company, or any other demonstrable material misconduct by Gershell or Daugherty, (2) ongoing and repeated failure or refusal to perform or neglect of his duties as required by his employment agreement, which failure, refusal or neglect continues for 30 days following receipt of written notice from the Company stating with specificity the nature of such failure, refusal or neglect, or (3) breach of any Company policy or any material provision of the Gershell Agreement or Daugherty Agreement, as applicable.
For purposes of the Agreements, “Good Reason” generally means (1) a material diminution in Executive’s title, authority, duties or responsibilities, (2) a material diminution in the executive officer’s base compensation, unless such a reduction is imposed across-the-board to the Company’s senior management, and for purposes of the Lederman Agreement, such reduction is not greater than 15%, (3) a material change in the geographic location at which the executive officer must perform his duties, (4) any other action or inaction that constitutes a material breach by the Company or any successor or affiliate of the Company’s obligations to Executive under the Agreement, or (5) the Company elects not to renew the Agreement for another term.
For purposes of the Agreements, “Change in Control” generally means:
|
|
· |
A transaction or series of transactions (other than public offerings) that results in any person or entity or related group of persons or entities (other than the Company, its subsidiaries, an employee benefit plan maintained by the Company or any of its subsidiaries or a person or entity that, prior to such transaction, directly or indirectly controls, is controlled by, or is under common control with, the Company) of beneficial ownership (within the meaning of Rule 13d-3 under the Exchange Act) of more than 40% of the total combined voting power of the Company’s securities outstanding immediately after such acquisition; |
|
|
· |
(1) a merger, consolidation, reorganization, or business combination or (2) the sale, exchange or transfer of all or substantially all of the Company’s assets in any single transaction or series of transactions or (3) the acquisition of assets or stock of another entity, in each case other than a transaction: |
|
|
· |
which results in the Company’s voting securities outstanding immediately before the transaction continuing to represent, directly or indirectly, at least 60% of the combined voting power of the successor entity’s outstanding voting securities immediately after the transaction, and |
|
|
· |
after which no person or group beneficially owns voting securities representing 40% or more of the combined voting power of the Company or its successor; provided, however, that no person or group is treated as beneficially owning 40% or more of combined voting power of the Company or its successor solely as a result of the voting power held in the Company prior to the consummation of the transaction. |
For purposes of the Agreements, “Enterprise Value” generally means (1) in a Change in Control in which consideration is received by the Company, the total cash and non-cash consideration, including debt assumed, received by the Company, net of any fees and expenses in connection with the transaction and (2) in a Change in Control in which consideration is payable to the stockholders of the Company, the total cash and non-cash consideration, including debt assumed, payable to the Company’s stockholders net of any fees and expenses in connection with the transaction. Enterprise Value also includes any cash or non-cash consideration payable to the Company or to the Company’s stockholders on a contingent, earnout or deferred basis.
Director Compensation
The following table sets forth summary information concerning the total compensation paid to our non-employee directors in 2013 for services to our company.
|
Name
|
|
Fees Earned
or Paid in
Cash ($)
|
|
Option
Awards ($)
|
|
Total ($)
|
|
|
Stuart Davidson
|
|
$
|
25,000
|
|
$
|
88,088
|
|
$
|
113,088
|
|
|
Patrick Grace
|
|
$
|
25,000
|
|
$
|
93,960
|
|
$
|
118,960
|
|
|
Donald Landry
|
|
$
|
25,000
|
|
$
|
82,215
|
|
$
|
107,215
|
|
|
Ernest Mario
|
|
$
|
25,000
|
|
$
|
82,215
|
|
$
|
107,215
|
|
|
Charles Mather IV
|
|
$
|
25,000
|
|
$
|
82,215
|
|
$
|
107,215
|
|
|
John Rhodes
|
|
$
|
25,000
|
|
$
|
88,088
|
|
$
|
113,088
|
|
|
Samuel Saks
|
|
$
|
25,000
|
|
$
|
82,215
|
|
$
|
107,215
|
|
|
Total:
|
|
$
|
175,000
|
|
$
|
598,995
|
|
$
|
773,995
|
|
ITEM 12- SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS
The following table sets forth certain information regarding beneficial ownership of our common stock as of March 24, 2014:
|
|
· |
by each person who is known by us to beneficially own more than 5% of our common stock; |
|
|
· by each of our officers and directors; and |
|
|
· by all of our officers and directors as a group. |
Unless otherwise indicated in the footnotes to the following table, each person named in the table has sole voting and investment power and that person’s address is c/o Tonix Pharmaceuticals Holding Corp., 509 Madison Avenue, Suite 306, New York New York 10022.
|
NAME OF OWNER
|
|
TITLE OF
CLASS
|
|
NUMBER OF
SHARES OWNED (1)
|
|
|
|
PERCENTAGE OF
COMMON STOCK (2)
|
|
|
Seth Lederman
|
|
Common Stock
|
|
531,437
|
|
(3)
|
|
5.29
|
%
|
|
Leland Gershell
|
|
Common Stock
|
|
54,021
|
|
(4)
|
|
*
|
|
|
Bruce Daugherty
|
|
Common Stock
|
|
138,998
|
|
(5)
|
|
1.39
|
%
|
|
Stuart Davidson
|
|
Common Stock
|
|
103,275
|
|
(6)
|
|
1.04
|
%
|
|
Patrick Grace
|
|
Common Stock
|
|
18,215
|
|
(7)
|
|
*
|
|
|
Donald Landry
|
|
Common Stock
|
|
96,057
|
|
(8)
|
|
*
|
|
|
Ernest Mario
|
|
Common Stock
|
|
188,651
|
|
(9)
|
|
1.89
|
%
|
|
Charles Mather IV
|
|
Common Stock
|
|
24,876
|
|
(10)
|
|
*
|
|
|
John Rhodes
|
|
Common Stock
|
|
113,320
|
|
(11)
|
|
1.14
|
%
|
|
Samuel Saks
|
|
Common Stock
|
|
47,813
|
|
(12)
|
|
*
|
|
|
Officers and Directors as a Group (10 persons)
|
|
Common Stock
|
|
1,271,539
|
|
(13)
|
|
12.27
|
%
|
|
|
|
|
|
|
|
|
|
|
|
|
Technology Partners Fund VIII, LP (14)
|
|
Common Stock
|
|
1,025,913
|
|
(15)
|
|
9.89
|
%
|
* Denotes less than 1%
(1) Beneficial Ownership is determined in accordance with the rules of the SEC and generally includes voting or investment power with respect to securities. Shares of common stock subject to options or warrants currently exercisable or convertible, or exercisable or convertible within 60 days of March 24, 2014 are deemed outstanding for computing the percentage of the person holding such option or warrant but are not deemed outstanding for computing the percentage of any other person.
(2) Percentage based upon 9,899,497 shares of common stock issued and outstanding as of March 24, 2014.
(3) Includes 51,456 shares of common stock underlying options which are currently exercisable or become exercisable within 60 days, 184,628 shares of common stock and 54,500 shares of common stock underlying warrants owned by Lederman & Co, 32,457 shares of common stock and 12,667 shares of common stock underlying warrants owned by L&L, 58,972 shares of common stock and 8,250 shares of common stock underlying warrants owned by Targent, 29,167 shares of common stock and 4,167 shares of common stock underlying warrants owned by Leder Laboratories, Inc. and 29,167 shares of common stock and 4,167 shares of common stock underlying warrants owned by Starling Pharmaceuticals, Inc. Seth Lederman, as the Managing Member of Lederman & Co and Targent, the Manager of L&L and the Chairman of Leder Laboratories, Inc. and Starling Pharmaceuticals, Inc., has investment and voting control over the shares held by these entities.
(4) Includes 38,536 shares of common stock underlying options which are currently exercisable or become exercisable within 60 days and 6,665 shares of common stock underlying warrants.
(5) Includes 25,838 shares of common stock underlying options which are currently exercisable or become exercisable within 60 days and 55,392 shares of common stock underlying warrants.
(6) Includes 11,359 shares of common stock underlying options which are currently exercisable or become exercisable within 60 days, 74,536 shares of common stock and 10,834 shares of common stock underlying warrants owned by Lysander, LLC and 6,546 shares owned by Oystercatcher Trust. Stuart Davidson, as the Member of Lysander, LLC and Trustee of Oystercatcher Trust, has investment and voting control over the shares held by these entities.
(7) Includes 11,669 shares of common stock underlying options which are currently exercisable or become exercisable within 60 days.
(8) Includes 11,046 shares of common stock underlying options which are currently exercisable or become exercisable within 60 days and 32,457 shares of common stock and 12,667 shares of common stock underlying warrants owned by L&L. Donald Landry, as a Member of L&L, has investment and voting control over the shares held by this entity.
(9) Includes 11,046 shares of common stock underlying options which are currently exercisable or become exercisable within 60 days and 57,892 shares of common stock underlying warrants.
(10) Includes 11,046 shares of common stock underlying options which are currently exercisable or become exercisable within 60 days and 3,000 shares of common stock underlying warrants.
(11) Includes 11,359 shares of common stock underlying options which are currently exercisable or become exercisable within 60 days and 26,765 shares of common stock underlying warrants.
(12) Includes 11,046 shares of common stock underlying options which are currently exercisable or become exercisable within 60 days and 14,217 shares of common stock underlying warrants.
(13) Includes 194,401 shares of common stock underlying options which are currently exercisable or become exercisable within 60 days, 184,628 shares of common stock and 54,500 shares of common stock underlying warrants owned by Lederman & Co, 32,457 shares of common stock and 12,667 shares of common stock underlying warrants owned by L&L, 58,972 shares of common stock and 8,250 shares of common stock underlying warrants owned by Targent, 29,167 shares of common stock and 4,167 shares of common stock underlying warrants owned by Leder Laboratories, Inc., 29,167 shares of common stock and 4,167 shares of common stock underlying warrants owned by Starling Pharmaceuticals, Inc., 74,536 shares of common stock and 10,834 shares of common stock underlying warrants owned by Lysander, LLC, 6,546 shares owned by Oystercatcher Trust and 176,936 shares of common stock underlying warrants owned directly by the executive officers and directors.
(14) The mailing address for this beneficial owner is 100 Shoreline Highway, Suite 282-B, Mill Valley, California 94941. Sheila Mutter and Roger Quy are the managing members of TP Management VIII, LLC, the general partner of Technology Partners Fund VIII, LP and have voting and investment power over the securities owned by it.
(15) Based upon a Schedule 13G/A dated as of December 31, 2013 and filed with the SEC on February 13, 2014 by Technology Partners Fund VIII, LP. Includes 477,941 shares of common stock underlying warrants. Does not include 1,333,334 purchased shares as of the January 2014 offering.
ITEM 13 - CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE
Other than as disclosed below, during the last two fiscal years, there have been no transactions, or proposed transactions, which have materially affected or will materially affect us in which any director, executive officer or beneficial holder of more than 5% of the outstanding common, or any of their respective relatives, spouses, associates or affiliates, has had or will have any direct or material indirect interest. We have no policy regarding entering into transactions with affiliated parties.
On June 4, 2010, Tonix Sub entered into a consulting agreement with Lederman & Co, of which our Chairman, CEO and President Seth Lederman is the Managing Member. Pursuant to this agreement, Lederman & Co shall provide clinical development, strategic, management and operational consulting services. In exchange for its services, Tonix Sub shall pay Lederman & Co compensation of $250,000 per annum and issued to Lederman & Co 261,784 shares of its common stock, 20% of which vested on the date of the agreement and the remainder vesting in equal amounts on each of the first, second, third and fourth anniversaries of the date of the agreement. On August 1, 2011, the cash compensation was reduced to $127,000 per annum. On February 1, 2012, the cash compensation was increased to $250,000 per annum. Immediately prior to the Share Exchange, the unvested shares of common stock vested.
On June 4, 2010, Tonix Sub entered into a consulting agreement with L&L, of which our Chairman, CEO and President Seth Lederman is the Manager. Pursuant to this agreement, L&L shall provide scientific and medical consulting services. In exchange for its services, Tonix Sub shall pay L&L compensation of $96,000 per annum, or such greater amount as the Board may designate from time to time, and issued to L&L 1,026,194 shares of its common stock, 25% of which vested on the date of the agreement and the remainder vesting in equal amounts on each of the first, second and third anniversaries of the date of the agreement. Immediately prior to the Share Exchange, the unvested shares of common stock vested.
On July 31, 2013, we sold a promissory note in the principal face amount of $150,000 to Lederman & Co., LLC in exchange for $150,000. The note is payable on demand at any time after one year from issuance and bears no interest.
On July 31, 2013, we sold a promissory note in the principal face amount of $50,000 to Eli Lederman in exchange for $50,000. The note is payable on demand at any time after one year from issuance and bears no interest.
On August 1, 2013, we sold a promissory note in the principal face amount of $80,000 to Lederman & Co., LLC in exchange for $80,000. The note is payable on demand at any time after one year from issuance and bears no interest.
ITEM 14 – PRINCIPAL ACCOUNTING FEES AND SERVICES
Audit Fees. The aggregate fees billed by our independent registered public accounting firm, for professional services rendered for the audit of our annual financial statements for the years ended December 31, 2013 and 2012, including review of our interim financial statements were $118,000 and $115,000, respectively.
Audit Related Fees. We incurred fees to our independent registered public accounting firm of $133,249 and $32,730 for audit related fees during the fiscal years ended December 31, 2013 and 2012, respectively, which related to filings with the SEC.
Tax and Other Fees. We incurred fees to our independent registered public accounting firm of $-0- for tax and fees during the fiscal years ended December 31, 2013 and 2012.
The Audit Committee pre-approves all auditing services and all permitted non-auditing services (including the fees and terms thereof) to be performed by our independent registered public accounting firm.
PART IV
ITEM 15 – EXHIBITS, FINANCIAL STATEMENT SCHEDULES
Exhibits:
|
2.01
|
Share Exchange Agreement, dated as of October 7, 2011 by and among Tamandare Explorations Inc., David J. Moss, Tonix Pharmaceuticals, Inc. and the shareholders of Tonix Pharmaceuticals, Inc. filed as an exhibit to the Current Report on Form 8-K, filed with the Commission on October 14, 2011 and incorporated herein by reference.
|
|
|
|
|
3.01
|
Articles of Incorporation, filed as an exhibit to the Registration Statement on Form S-1, filed with the Securities and Exchange Commission (the “Commission”) on April 9, 2008 and incorporated herein by reference.
|
|
|
|
|
3.02
|
Articles of Merger between Tamandare Explorations Inc. and Tonix Pharmaceuticals Holding Corp., effective October 11, 2011, filed as an exhibit to the Current Report on Form 8-K, filed with the Commission on October 17, 2011 and incorporated herein by reference.
|
|
|
|
|
3.03
|
Amended and Restated Bylaws, filed as an exhibit to the Current Report on Form 8-K, filed with the Commission on February 23, 2012 and incorporated herein by reference.
|
|
|
|
|
10.01
|
Lease Agreement, dated as of September 28, 2010, by and between 509 Madison Avenue Associates, L.P. and Tonix Pharmaceuticals, Inc., filed as an exhibit to the amended Current Report on Form 8-K/A, filed with the Commission on February 3, 2012 and incorporated herein by reference.
|
|
|
|
|
10.02
|
Form of Class A Warrant, filed as an exhibit to the Current Report on Form 8-K, filed with the Commission on January 23, 2012 and incorporated herein by reference.
|
|
|
|
|
10.03
|
Form of Class B Warrant, filed as an exhibit to the Current Report on Form 8-K, filed with the Commission on January 23, 2012 and incorporated herein by reference.
|
|
|
|
|
10.04
|
Form of Registration Rights Agreement, dated January 20, 2012, filed as an exhibit to the Current Report on Form 8-K, filed with the Commission on January 23, 2012 and incorporated herein by reference.
|
|
|
|
|
10.05
|
Employment Agreement, between Tonix Pharmaceuticals Holding Corp. and Leland Gershell, dated April 1, 2012, filed as an exhibit to the Current Report on Form 8-K filed with the Commission on April 5, 2012 and incorporated herein by reference.
|
|
|
|
|
10.06
|
Employment Agreement, between Tonix Pharmaceuticals Holding Corp. and Benjamin Selzer, dated April 2, 2012, filed as an exhibit to the Current Report on Form 8-K filed with the Commission on April 5, 2012 and incorporated herein by reference.
|
|
|
|
|
10.07
|
Amendment to Employment Agreement, between Tonix Pharmaceuticals Holding Corp. and Benjamin Selzer, dated October 5, 2012, filed as an exhibit to the Current Report on Form 8-K filed with the Commission on October 10, 2012 and incorporated herein by reference.
|
|
|
|
|
10.08
|
Form of Subscription Agreement, dated November 13, 2012, filed as an exhibit to the Current Report on Form 8-K filed with the Commission on November 14, 2012 and incorporated herein by reference.
|
|
|
|
|
10.09
|
Form of Convertible Debenture, dated November 13, 2012, filed as an exhibit to the Current Report on Form 8-K filed with the Commission on November 14, 2012 and incorporated herein by reference.
|
|
|
|
|
10.10
|
Form of Subscription Agreement, dated December 2012, filed as an exhibit to the Current Report on Form 8-K filed with the Commission on December 5, 2012 and incorporated herein by reference.
|
|
|
|
|
10.11
|
Form of Class A Warrant, dated December 4, 2012, filed as an exhibit to the Current Report on Form 8-K filed with the Commission on December 5, 2012 and incorporated herein by reference.
|
|
|
|
|
10.12
|
Form of Class B Warrant, dated December 4, 2012, filed as an exhibit to the Current Report on Form 8-K filed with the Commission on December 5, 2012 and incorporated herein by reference.
|
|
10.13
|
Form of Registration Rights Agreement, dated December 2012, filed as an exhibit to the Current Report on Form 8-K filed with the Commission on December 5, 2012 and incorporated herein by reference.
|
|
|
|
|
10.14
|
Form of Class A Warrant, dated December 21, 2012, filed as an exhibit to the Current Report on Form 8-K filed with the Commission on December 27, 2012 and incorporated herein by reference.
|
|
|
|
|
10.15
|
Form of Class B Warrant, dated December 21, 2012, filed as an exhibit to the Current Report on Form 8-K filed with the Commission on December 27, 2012 and incorporated herein by reference.
|
|
|
|
|
10.16
|
Form of Amendment No. 1 to the Purchase Agreement, Registration Rights Agreement and Escrow Agreement, filed as an exhibit to the Current Report on Form 8-K filed with the Commission on December 27, 2012 and incorporated herein by reference.
|
|
|
|
|
10.17
|
Form of Demand Promissory Note, filed as an exhibit to the amended registration statement on Form S-1/A filed with the Commission on August 8, 2013 and incorporated herein by reference.
|
|
|
|
|
10.18
|
Amendment to Consulting Agreement, between Tonix Pharmaceuticals, Inc. and Lederman & Co., LLC, dated October 15, 2013, filed as an exhibit to the Current Report on Form 8-K filed with the Commission on October 17, 2013 and incorporated herein by reference.
|
|
|
|
|
10.19
|
Amendment to Employment Agreement, between Tonix Pharmaceuticals Holding Corp. and Leland Gershell, dated October 15, 2013, filed as an exhibit to the Current Report on Form 8-K filed with the Commission on October 17, 2013 and incorporated herein by reference.
|
|
|
|
|
10.20
|
Amendment to Employment Agreement, between Tonix Pharmaceuticals Holding Corp. and Bruce Daugherty, dated October 15, 2013, filed as an exhibit to the Current Report on Form 8-K filed with the Commission on October 17, 2013 and incorporated herein by reference.
|
|
|
|
|
10.21
|
Employment Agreement, between Tonix Pharmaceuticals Holding Corp. and Seth Lederman, dated February 11, 2014, filed as an exhibit to the Current Report on Form 8-K filed with the Commission on February 14, 2014 and incorporated herein by reference.
|
|
|
|
|
10.22
|
Letter of Termination, between Tonix Pharmaceuticals Holding Corp. and Lederman & Co., LLC, dated February 11, 2014, filed as an exhibit to the Current Report on Form 8-K filed with the Commission on February 14, 2014 and incorporated herein by reference.
|
|
|
|
|
14.01
|
Code of Ethics and Business Conduct for Officers, Directors and Employees, filed as an exhibit to the Current Report on Form 8-K, filed with the Commission on February 23, 2012 and incorporated herein by reference.
|
|
|
|
|
21.01
|
List of Subsidiaries, filed as an exhibit to the registration statement on Form S-1 filed with the Commission on May 10, 2013 and incorporated herein by reference.
|
|
|
|
|
23.01
|
Consent of Independent Registered Public Accounting Firm.
|
|
|
|
|
31.01
|
Certification of Chief Executive Officer pursuant to Exchange Act Rules 13a-14(a) and 15d-14(a), as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002.
|
|
|
|
|
31.02
|
Certification of Chief Financial Officer pursuant to Exchange Act Rules 13a-14(a) and 15d-14(a), as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002.
|
|
|
|
|
32.01
|
Certifications of Chief Executive Officer and Chief Financial Officer pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002.
|
|
|
|
|
101 INS
|
XBRL Instance Document
|
|
|
|
|
101 SCH
|
XBRL Taxonomy Extension Schema Document
|
|
|
|
|
101 CAL
|
XBRL Taxonomy Calculation Linkbase Document
|
|
|
|
|
101 LAB
|
XBRL Taxonomy Labels Linkbase Document
|
|
|
|
|
101 PRE
|
XBRL Taxonomy Presentation Linkbase Document
|
|
|
|
|
101 DEF
|
XBRL Taxonomy Extension Definition Linkbase Document
|
SIGNATURES
In accordance with the requirements of the Exchange Act, the registrant caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
|
|
TONIX PHARMACEUTICALS HOLDING CORP.
|
|
|
|
|
|
|
|
Date: March 28, 2014
|
By:
|
/s/ SETH LEDERMAN
|
|
|
|
|
Seth Lederman
|
|
|
|
|
Chief Executive Officer (Principal Executive
Officer)
|
|
|
|
|
|
|
|
Date: March 28, 2014
|
By:
|
/s/ LELAND GERSHELL
|
|
|
|
|
Leland Gershell
|
|
|
|
|
Chief Financial Officer (Principal Financial Officer and Principal Accounting Officer)
|
|
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
|
Name
|
|
Position
|
|
Date
|
|
|
|
|
|
|
|
/s/ SETH LEDERMAN
|
|
Director
|
|
March 28, 2014
|
|
Seth Lederman
|
|
|
|
|
|
|
|
|
|
|
|
/s/ STUART DAVIDSON
|
|
Director
|
|
March 28, 2014
|
|
Stuart Davidson
|
|
|
|
|
|
|
|
|
|
|
|
/s/ PATRICK GRACE
|
|
Director
|
|
March 28, 2014
|
|
Patrick Grace
|
|
|
|
|
|
|
|
|
|
|
|
/s/ DONALD W. LANDRY
|
|
Director
|
|
March 28, 2014
|
|
Donald W. Landry
|
|
|
|
|
|
|
|
|
|
|
|
/s/ ERNEST MARIO
|
|
Director
|
|
March 28, 2014
|
|
Ernest Mario
|
|
|
|
|
|
|
|
|
|
|
|
/s/ CHARLES MATHER IV
|
|
Director
|
|
March 28, 2014
|
|
Charles Mather IV
|
|
|
|
|
|
|
|
|
|
|
|
/s/ JOHN RHODES
|
|
Director
|
|
March 28, 2014
|
|
John Rhodes
|
|
|
|
|
|
|
|
|
|
|
|
/s/ SAMUEL SAKS
|
|
Director
|
|
March 28, 2014
|
|
Samuel Saks
|
|
|
|
|