Exhibit 99.01
© Copyright 2016 Tonix Pharmaceuticals - Confidential - Do not duplicate or distribute NASDAQ: TNXP Investor Presentation September 2016 © 2016 Tonix Pharmaceuticals Holding Corp. Version : P0029 09 - 19 - 2016
2 © Copyright 2016 Tonix Pharmaceuticals Cautionary note on forward - looking statements Certain statements in this presentation regarding strategic plans, expectations and objectives for future operations or results are “forward - looking statements” as defined by the Private Securities Litigation Reform Act of 1995 . These statements may be identified by the use of forward - looking words such as “anticipate,” “believe,” “forecast,” “estimate,” and “intend,” among others . These forward - looking statements are based on Tonix’s current expectations and actual results could differ materially . There are a number of factors that could cause actual events to differ materially from those indicated by such forward - looking statements . These factors include, but are not limited to, substantial competition ; our need for additional financing ; uncertainties of patent protection and litigation ; uncertainties of government or third party payor reimbursement ; limited research and development efforts and dependence upon third parties ; and risks related to failure to obtain U . S . Food and Drug Administration clearances or approvals and noncompliance with its regulations . As with any pharmaceutical under development, there are significant risks in the development, regulatory approval and commercialization of new products . The forward - looking statements in this presentation are made as of the date of this presentation, even if subsequently made available by the Company on its website or otherwise . Tonix does not undertake an obligation to update or revise any forward - looking statement, except as required by law . Investors should read the risk factors set forth in the Annual Report on Form 10 - K for the year ended December 31 , 2015 , as filed with the Securities and Exchange Commission (the “SEC”) on March 3 , 2016 , and future periodic reports filed with the SEC on or after the date hereof . All of the Company's forward - looking statements are expressly qualified by all such risk factors and other cautionary statements .
3 © Copyright 2016 Tonix Pharmaceuticals Developing innovative medicines for large and growing markets • Targeting common central nervous system disorders ‒ One clinical - stage proprietary candidate targeting posttraumatic stress disorder (PTSD ) ‒ Differentiated product with potential for sustainable competitive advantages • PTSD – Phase 2 trial reported May 2016 ‒ TNX - 102 SL 1 5.6 mg was active in treating military - related PTSD ‒ Serious mental health problem 2 ‒ Planning Phase 3 trial in military - related PTSD • All intellectual property owned by Tonix 2 Schnurr , PP et al., Contemporary Clinical Trials 2015;41:75. 1 T NX - 102 SL (cyclobenzaprine HCl sublingual tablets ) is an Investigational New Drug and is not approved for any indication.
4 © Copyright 2016 Tonix Pharmaceuticals Overview: PTSD program • Results from multi - center, double - blind, randomized, placebo - controlled Phase 2 trial in military - related PTSD reported May 2016 ‒ Optimal therapeutic dose identified ‒ TNX - 102 SL 5.6 mg was active in treating military - related PTSD ‒ Reduction in symptoms and disease severity [( Clinician - Administered PTSD Scale) CAPS - 5] ‒ Improvement in clinical global impression (CGI - I) ‒ Improvement in function (Sheehan Disability Scale domains for work/school and social/leisure) ‒ Systemic side effects include somnolence, dry mouth, headache and sedation ‒ A dministrative site reactions were common (transient tongue numbness) ‒ Completion rate for TNX - 102 SL 5.6 mg was 84% and for placebo was 73% • Phase 3 program planned ‒ U.S. Food and Drug Administration (FDA) acceptance of proposed Phase 3 program at August 2016 EOP2/Pre - Phase 3 meeting ‒ TNX - 102 SL 5.6 mg is the appropriate dose for confirmatory study ‒ An adaptive design Phase 3 study in military - related PTSD similar to AtEase is being planned Q1 2017 ‒ CAPS - 5 enrollment threshold will be changed from ≥ 29 to ≥ 33 • Potential for Breakthrough Therapy Designation
5 © Copyright 2016 Tonix Pharmaceuticals Tonix is developing TNX - 102 SL for PTSD • Advanced sublingual tablet containing low - dose cyclobenzaprine (CBP) ‒ Designed for daily bedtime administration with no titration ‒ Efficient transmucosal absorption ‒ Avoidance of first - pass metabolism reduces formation of long - lived metabolite • TNX - 102 SL’s pharmacologic action is believed to improve sleep quality ‒ Disturbed sleep is a common clinical feature of PTSD ‒ TNX - 102 SL targets receptors believed to play key roles in sleep physiology • Phase 2 “ AtEase ” study was successfully completed in May 2016 • FDA acceptance of Phase 3 proposal and product registration plan in August 2016
6 © Copyright 2016 Tonix Pharmaceuticals PTSD is a chronic stress disorder triggered by a traumatic event • PTSD is characterized by: • Considered a stress response, but prolonged and does not resolve with time ‒ 20% of women and 8% of men in the U.S. who experience significant trauma develop PTSD 1 • Associated with significant life disruption ‒ Social isolation, inability to maintain employment, loss of independent living ‒ Unpredictable acts of violence, suicidal thoughts – Re - experiencing the triggering event – Negative alterations in mood/cognition – Situation/stimulus avoidance – Hyperarousal (anxiety, agitation & sleep disturbance) 1 Kessler et al, Arch Gen Psychiatry 1995;52:1048.
7 © Copyright 2016 Tonix Pharmaceuticals PTSD is a prevalent problem for both civilians and the military • ~70% are considered to have moderate to severe symptoms • Of those diagnosed, ~50% utilize professional healthcare (psychotherapy/pharmacotherapy) 2 1 Kessler RC at al, Arch Gen Psychiatry 2005;62:617; U.S. Census Bureau, 2013 Projection. 2 Wang et al, Arch Gen Psychiatry 2005;62:629. 3 Report on VA Facility Specific Operation Enduring Freedom (OEF), Operation Iraqi Freedom (OIF), and Operation New Dawn (OND) Veterans Diagnosed with Potential or Provisional PTSD. 4 Bowe et al, J Dual Diagnosis 2015;11:22. Affects 3.5% (8.5 M) U.S. Adults 1 • Higher prevalence in military population - 20% of veterans from recent conflicts will have potential/provisional PTSD 3 - ~638,000 veterans with PTSD in the Veterans Affairs (VA) health system (2012) 4 - Majority are male - Alcohol and substance abuse are common
8 © Copyright 2016 Tonix Pharmaceuticals Limitations of current FDA - approved pharmacotherapies for military - related PTSD • No treatment response observed in U.S. military population ‒ Sertraline: negative large multi - center trial in U.S. military veterans 1 ‒ Placebo numerically superior on CAPS - 2 ‒ Paroxetine: not studied in military population • Inconsistent treatment response observed in males ‒ Sertraline: FDA - conducted post - hoc analysis concluded no effect for male civilian subgroup 2 ‒ Paroxetine: no gender - related difference in treatment outcome 3 • Important tolerability considerations with SSRIs in this population ‒ Sexual dysfunction ‒ Insomnia SSRI: Selective Serotonin Reuptake Inhibitor. 1 Friedman MJ et al. J Clin Psychiatry 2007;68:711 - 20. 2 Zoloft® Package Insert, Pfizer, August 2014. 3 Paxil® Package Insert, Glaxo, June 2014.
9 © Copyright 2016 Tonix Pharmaceuticals Phase 2 AtEase study of TNX - 102 SL in PTSD AtEase Study • Randomized, double - blind, placebo - controlled trial • DSM - 5 diagnostic criteria for PTSD • 231* participants studied 2:1:2 at 24 U.S. sites ‒ 1 x TNX - 102 SL 2.8 mg tablet: 2 x TNX - 102 SL 2.8 mg tablets: placebo • Evaluated the Clinician Administered PTSD Scale for DSM - 5 (CAPS - 5) as primary endpoint ‒ Pre - specified primary analysis was 2.8 mg dose *Modified intent - to - treat ( mITT ) population
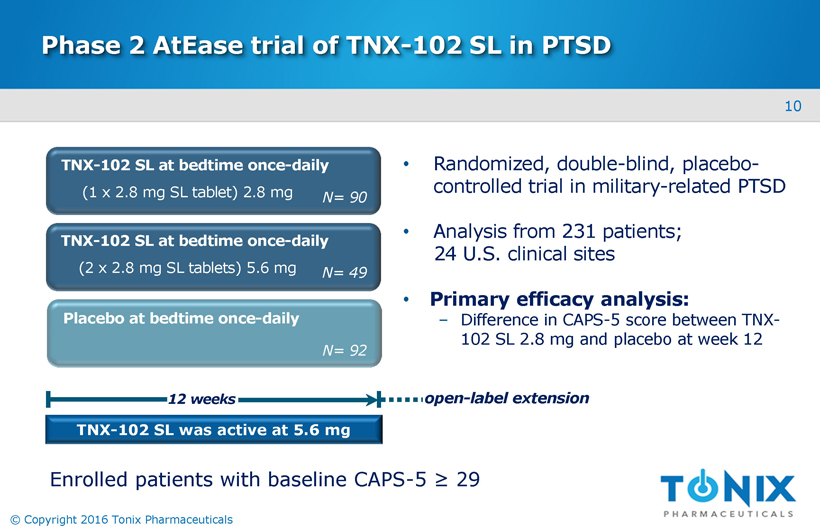
10 © Copyright 2016 Tonix Pharmaceuticals Phase 2 AtEase trial of TNX - 102 SL in PTSD • Randomized, double - blind, placebo - controlled trial in military - related PTSD • Analysis from 231 patients; 24 U.S. clinical sites • Primary efficacy analysis: ‒ Difference in CAPS - 5 score between TNX - 102 SL 2.8 mg and placebo at week 12 TNX - 102 SL was act ive at 5.6 mg TNX - 102 SL at bedtime once - daily Placebo at bedtime once - daily 12 weeks N= 90 TNX - 102 SL at bedtime once - daily N= 92 N= 49 (1 x 2.8 mg SL tablet) 2.8 mg (2 x 2.8 mg SL tablets) 5.6 mg open - label extension Enrolled patients with baseline CAPS - 5 ≥ 29
11 © Copyright 2016 Tonix Pharmaceuticals AtEase study of TNX - 102 SL in PTSD Key Demographics / Characteristics of AtEase • 93% of the patients were male • 98% had trauma during military service and were deployed on average 2.3 times • Mean time since index trauma was 7 years • Race and ethnicity generally consistent with U.S. military distribution • Similar baseline CAPS - 5 scores and MADRS 1 scores across treatment arms ‒ Average CAPS - 5 scores were greater than 39 for all groups ('severe' PTSD 2 ) 1 Montgomery – Åsberg Depression Rating Scale 2 personal communication – Frank Weathers PhD, National Center for PTSD
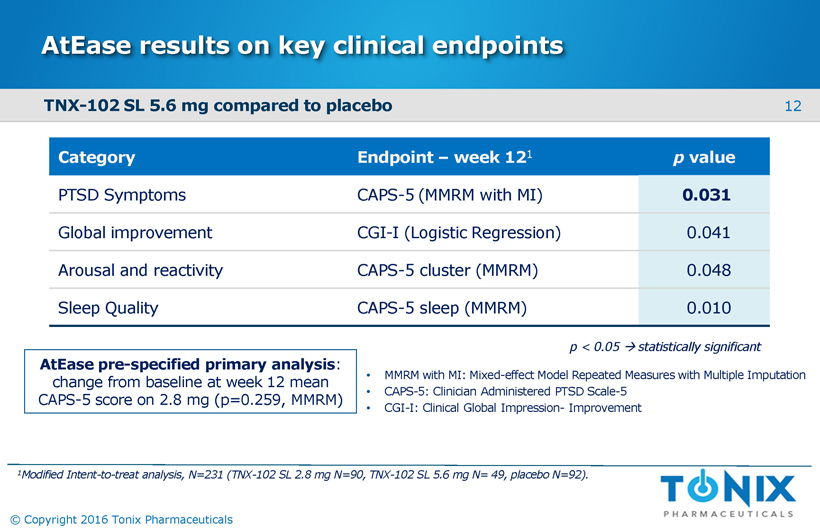
12 © Copyright 2016 Tonix Pharmaceuticals AtEase results on key clinical endpoints Category Endpoint – week 12 1 p value PTSD Symptoms CAPS - 5 (MMRM with MI) 0.031 Global improvement CGI - I (Logistic Regression) 0.041 Arousal and reactivity CAPS - 5 cluster (MMRM) 0.048 Sleep Quality CAPS - 5 sleep (MMRM) 0.010 AtEase pre - specified primary analysis : change from baseline at week 12 mean CAPS - 5 score on 2.8 mg (p=0.259, MMRM) • MMRM with MI: Mixed - effect Model Repeated Measures with Multiple Imputation • CAPS - 5: Clinician Administered PTSD Scale - 5 • CGI - I: Clinical Global Impression - Improvement p < 0.05 statistically significant 1 Modified Intent - to - treat analysis, N=231 (TNX - 102 SL 2.8 mg N=90, TNX - 102 SL 5.6 mg N= 49, placebo N=92). TNX - 102 SL 5.6 mg compared to placebo
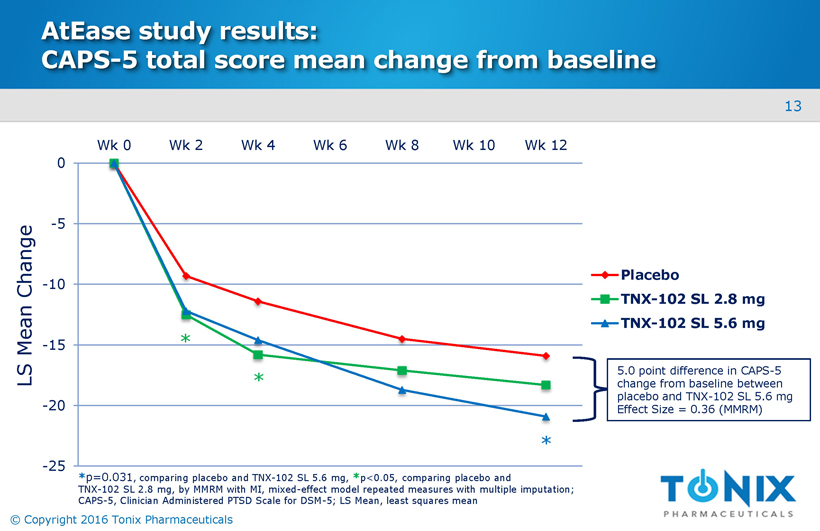
13 © Copyright 2016 Tonix Pharmaceuticals AtEase study results: CAPS - 5 total score mean change from baseline -25 -20 -15 -10 -5 0 Wk 0 Wk 2 Wk 4 Wk 6 Wk 8 Wk 10 Wk 12 Placebo TNX-102 SL 2.8 mg TNX-102 SL 5.6 mg * * p=0.031 , comparing placebo and TNX - 102 SL 5.6 mg, * p<0.05, comparing placebo and TNX - 102 SL 2.8 mg, by MMRM with MI, mixed - effect model repeated measures with multiple imputation; CAPS - 5, Clinician Administered PTSD Scale for DSM - 5; LS Mean, least squares mean LS Mean Change * * 5.0 point difference in CAPS - 5 change from baseline between placebo and TNX - 102 SL 5.6 mg Effect Size = 0.36 (MMRM)
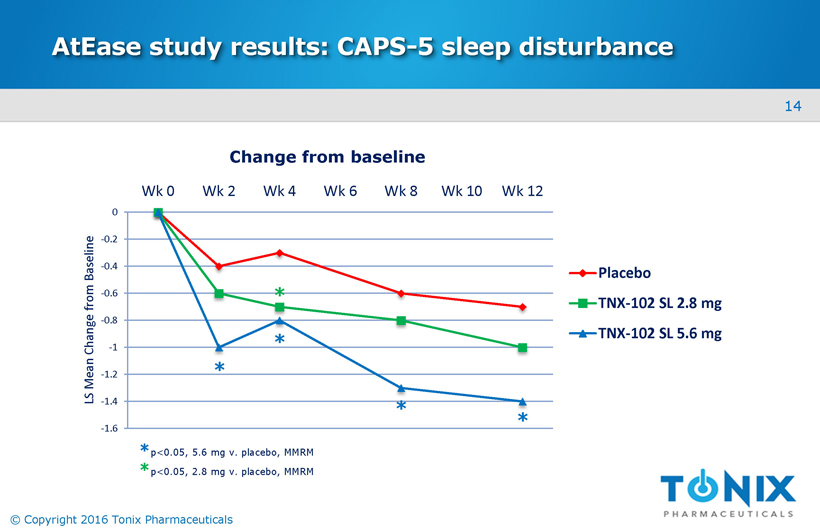
14 © Copyright 2016 Tonix Pharmaceuticals AtEase study results: CAPS - 5 sleep disturbance -1.6 -1.4 -1.2 -1 -0.8 -0.6 -0.4 -0.2 0 Wk 0 Wk 2 Wk 4 Wk 6 Wk 8 Wk 10 Wk 12 LS Mean Change from Baseline Placebo TNX-102 SL 2.8 mg TNX-102 SL 5.6 mg Change from baseline * * * * * p<0.05, 5.6 mg v. placebo, MMRM * p<0.05, 2.8 mg v. placebo, MMRM *
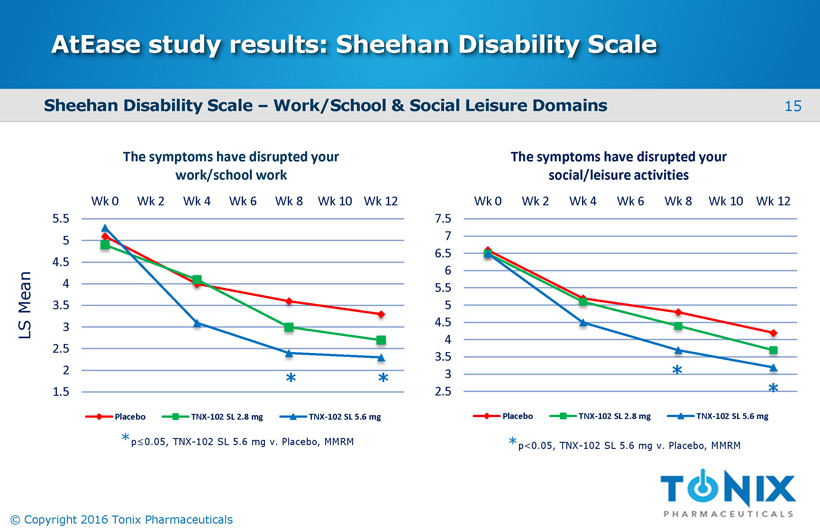
15 © Copyright 2016 Tonix Pharmaceuticals AtEase study results: Sheehan Disability Scale 1.5 2 2.5 3 3.5 4 4.5 5 5.5 Wk 0 Wk 2 Wk 4 Wk 6 Wk 8 Wk 10 Wk 12 The symptoms have disrupted your work/school work Placebo TNX-102 SL 2.8 mg TNX-102 SL 5.6 mg 2.5 3 3.5 4 4.5 5 5.5 6 6.5 7 7.5 Wk 0 Wk 2 Wk 4 Wk 6 Wk 8 Wk 10 Wk 12 The symptoms have disrupted your social/leisure activities Placebo TNX-102 SL 2.8 mg TNX-102 SL 5.6 mg * * * * * p≤0.05, TNX - 102 SL 5.6 mg v. Placebo, MMRM * p<0.05, TNX - 102 SL 5.6 mg v. Placebo, MMRM Sheehan Disability Scale – Work/School & Social Leisure Domains LS Mean
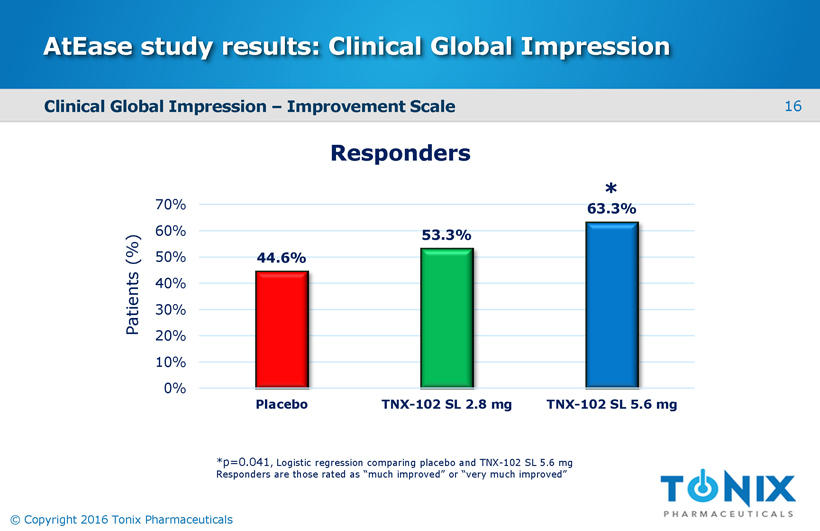
16 © Copyright 2016 Tonix Pharmaceuticals AtEase study results: Clinical Global Impression 44.6% 53.3% 63.3% 0% 10% 20% 30% 40% 50% 60% 70% Placebo TNX-102 SL 2.8 mg TNX-102 SL 5.6 mg * *p=0.041 , Logistic regression comparing placebo and TNX - 102 SL 5.6 mg Responders are those rated as “much improved” or “very much improved” Responders Clinical Global Impression – Improvement Scale Patients (%)
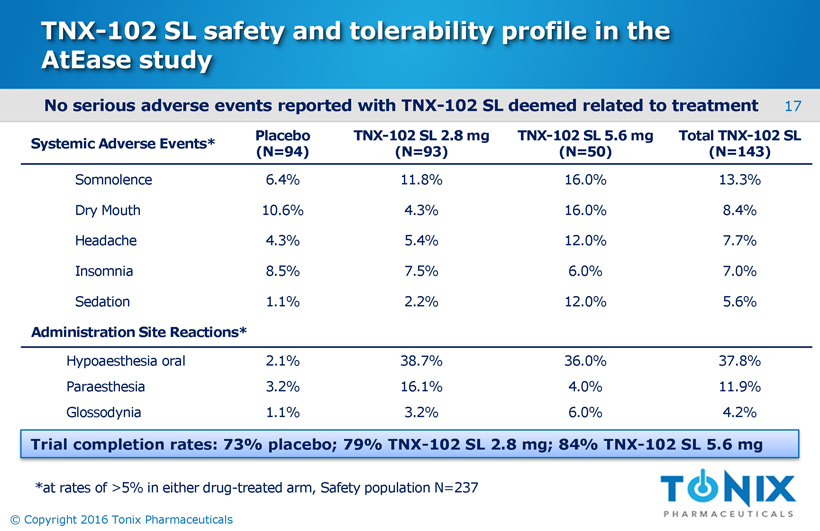
17 © Copyright 2016 Tonix Pharmaceuticals TNX - 102 SL safety and tolerability profile in the AtEase study No serious adverse events reported with TNX - 102 SL deemed related to treatment Systemic Adverse Events* Placebo (N=94) TNX - 102 SL 2.8 mg (N=93) TNX - 102 SL 5.6 mg (N=50) Total TNX - 102 SL (N=143) Somnolence 6.4% 11.8% 16.0% 13.3% Dry Mouth 10.6% 4.3% 16.0% 8.4% Headache 4.3% 5.4% 12.0% 7.7% Insomnia 8.5% 7.5% 6.0% 7.0% Sedation 1.1% 2.2% 12.0% 5.6% Administration Site Reactions* Hypoaesthesia oral 2.1% 38.7% 36.0% 37.8% Paraesthesia 3.2% 16.1% 4.0% 11.9% Glossodynia 1.1% 3.2% 6.0% 4.2% Trial completion rates: 73% placebo; 79% TNX - 102 SL 2.8 mg; 84% TNX - 102 SL 5.6 mg *at rates of >5% in either drug - treated arm, Safety population N=237
18 © Copyright 2016 Tonix Pharmaceuticals Determining CAPS - 5 severity criteria for entry in phase 3 trials • CAPS - 5 has not been employed previously in a pharmacotherapy trial ; entry severity threshold not clear ; ≥ 29 used in the Phase 2 AtEase study • Prior pharmacotherapy trials in PTSD using earlier versions of CAPS with different scoring range have most frequently used a score of ≥ 50 for entry (similar to CAPS - 5 ≥ 33 1 ) • Analysis of patients with CAPS - 5 ≥ 33 showed an effect size of 0 . 53 on mean change from baseline at Week 12 in TNX - 102 SL 5 . 6 mg group (see figure on next slide) 1 Sullivan, Gregory, et al. “The AtEase Study: Efficacy and Safety of a Low Dose, Bedtime, Sublingual Formulation of Cyclobenzaprine (TNX - 102 SL) for the Treatment of Military - Related PTSD.” Poster session presented at: Military Health System Research Symposium (MHSRS) 2016 Annual Meeting; 2016 Aug 15 - 18; Kissimmee, FL. URL: http://bit.ly/2bFo4mx
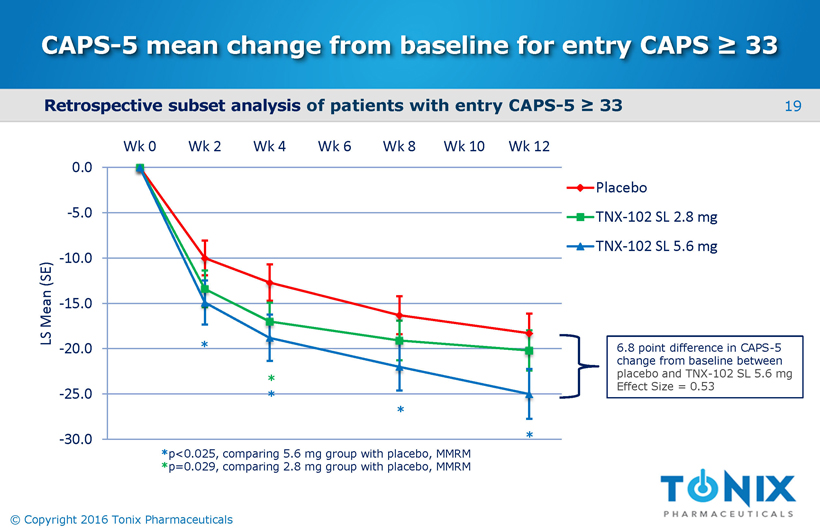
19 © Copyright 2016 Tonix Pharmaceuticals CAPS - 5 mean change from baseline for entry CAPS ≥ 33 -30.0 -25.0 -20.0 -15.0 -10.0 -5.0 0.0 Wk 0 Wk 2 Wk 4 Wk 6 Wk 8 Wk 10 Wk 12 LS Mean (SE) Placebo TNX-102 SL 2.8 mg TNX-102 SL 5.6 mg 6.8 point difference in CAPS - 5 change from baseline between placebo and TNX - 102 SL 5.6 mg Effect Size = 0.53 * * * * * * p<0.025, comparing 5.6 mg group with placebo, MMRM * p=0.029, comparing 2.8 mg group with placebo, MMRM Retrospective subset analysis of patients with entry CAPS - 5 ≥ 33
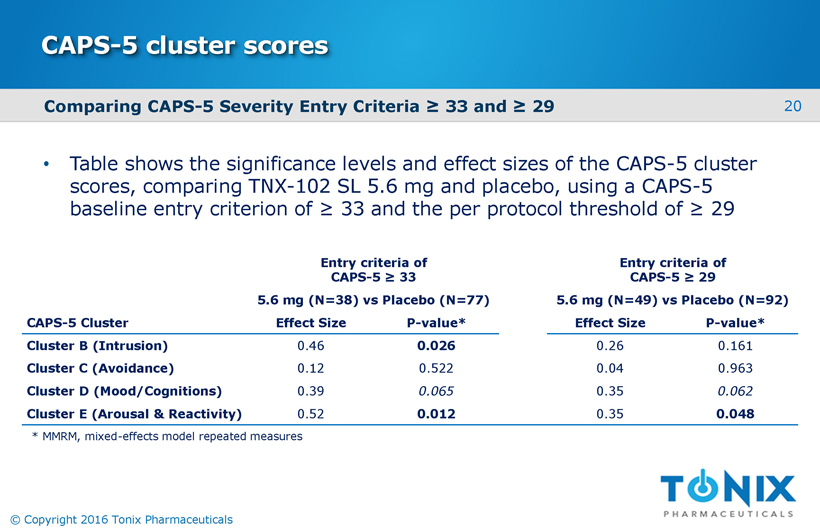
20 © Copyright 2016 Tonix Pharmaceuticals CAPS - 5 cluster scores • Table shows the significance levels and effect sizes of the CAPS - 5 cluster scores, comparing TNX - 102 SL 5.6 mg and placebo, using a CAPS - 5 baseline entry criterion of ≥ 33 and the per protocol threshold of ≥ 29 Entry criteria of CAPS - 5 ≥ 33 Entry criteria of CAPS - 5 ≥ 29 5.6 mg (N=38) vs Placebo (N=77) 5.6 mg (N=49) vs Placebo (N=92) CAPS - 5 Cluster Effect Size P - value* Effect Size P - value* Cluster B (Intrusion) 0.46 0.026 0.26 0.161 Cluster C (Avoidance) 0.12 0.522 0.04 0.963 Cluster D (Mood/Cognitions) 0.39 0.065 0.35 0.062 Cluster E (Arousal & Reactivity) 0.52 0.012 0.35 0.048 * MMRM, mixed - effects model repeated measures Comparing CAPS - 5 Severity Entry Criteria ≥ 33 and ≥ 29
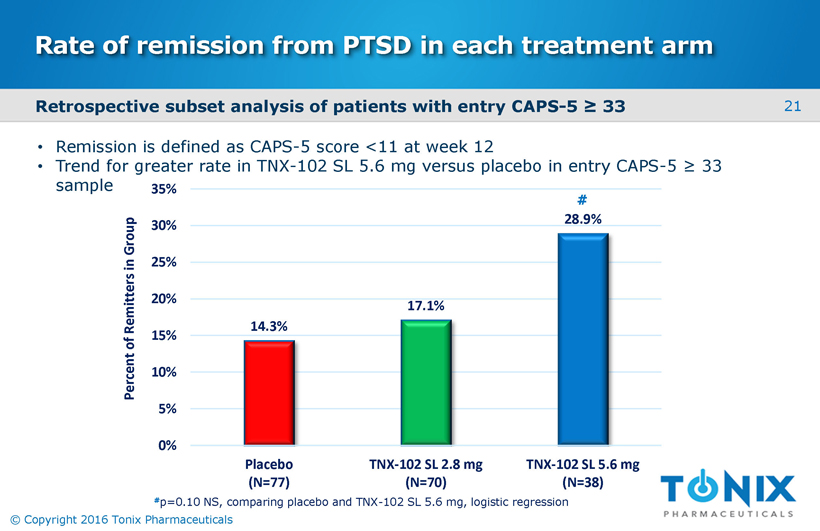
21 © Copyright 2016 Tonix Pharmaceuticals Rate of remission from PTSD in each treatment arm 14.3% 17.1% 28.9% 0% 5% 10% 15% 20% 25% 30% 35% Placebo (N=77) TNX-102 SL 2.8 mg (N=70) TNX-102 SL 5.6 mg (N=38) Percent of Remitters in Group # p=0.10 NS, comparing placebo and TNX - 102 SL 5.6 mg, logistic regression # • Remission is defined as CAPS - 5 score <11 at week 12 • Trend for greater rate in TNX - 102 SL 5.6 mg versus placebo in entry CAPS - 5 ≥ 33 sample Retrospective subset analysis of patients with entry CAPS - 5 ≥ 33
22 © Copyright 2016 Tonix Pharmaceuticals AtEase study conclusions • This Phase 2 trial is the first large multi - center trial of an investigational new drug product that demonstrated efficacy in a population with military - related PTSD ‒ Symptom reduction (CAPS - 5) ‒ Functional improvement (Sheehan Disability Scale domains) ‒ Global improvement (CGI - I) • Early effects on sleep and hyperarousal are consistent with the mechanistic hypothesis of TNX - 102 SL primary actions on sleep disturbance and autonomic balance • Systemic side effects included include somnolence, dry mouth, headache and sedation; local reactions to sublingual TNX - 102 SL administration were common (transient tongue numbness) • A post - hoc analysis suggested that enrolling patients with a higher CAPS - 5 score (≥ 33) would be similar to the entry criteria used in the registration studies supporting the approval of the marketed PTSD drug products ‒ Same post - hoc analysis revealed a larger separation from placebo in the subset of patients with baseline CAPS - 5 ≥ 33 at weeks 2, 4, 8 and 12 ‒ Phase 3 program will use CAPS - 5 ≥ 33 as enrollment threshold
23 © Copyright 2016 Tonix Pharmaceuticals Planned Phase 3 program in PTSD General Study Characteristics: • Randomized, double - blind, placebo - controlled, entrance CAPS - 5 > 33 • At least one unblinded interim analyses (IA) • First IA (N ~180) for efficacy stop, futility or sample size adjustment • Potential to enroll 550 patients • Approximately 25 U.S. clinical sites Primary Efficacy Endpoint: • Mean change from baseline in total CAPS - 5 at Week 12 compared between TNX - 102 SL 5.6 mg and placebo Placebo once - daily at bedtime 12 weeks TNX - 102 SL once - daily at bedtime N ~ 90* N ~ 90* 5.6 mg First IA topline data anticipated 2H 2017 To confirm AtEase finding in military - related PTSD: • Larger adaptive design study • Targeting start in Q1 2017 * First interim analysis
24 © Copyright 2016 Tonix Pharmaceuticals Intellectual property • Composition - of - matter (eutectic) ‒ Patents filed ‒ Protection expected to 2034 • Pharmacokinetics (PK) ‒ Patents filed ‒ Protection expected to 2033 • Method - of - use ‒ PTSD : patents filed TNX - 102 SL Wholly - owned by Tonix with no obligations to others
25 © Copyright 2016 Tonix Pharmaceuticals TNX - 102 SL: active pharmaceutical ingredient • Cyclobenzaprine is a tricyclic molecule that binds to a number of central nervous system (CNS) receptor types • Highest affinity for three receptors believed to have a role in treating sleep disturbances ‒ 5 - HT 2A receptor ‒ a 1 adrenergic receptor ‒ H 1 receptor
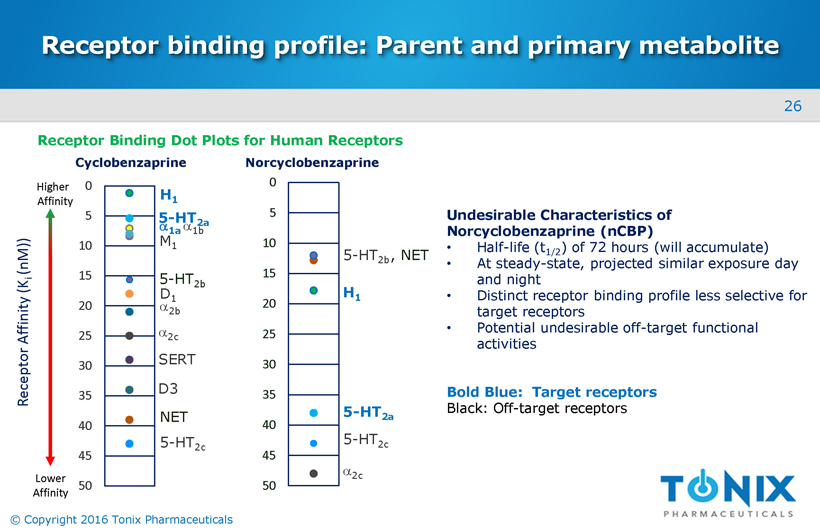
26 © Copyright 2016 Tonix Pharmaceuticals Receptor binding profile: Parent and primary metabolite 0 5 10 15 20 25 30 35 40 45 50 5 - HT 2c H 1 5 - HT 2a a 2 c , NET 5 - HT 2b Undesirable Characteristics of Norcyclobenzaprine (nCBP) • Half - life (t 1/2 ) of 72 hours (will accumulate) • At steady - state, projected similar exposure day and night • Distinct receptor binding profile less selective for target receptors • Potential undesirable off - target functional activities Bold Blue: Target receptors Black: Off - target receptors Lower Affinity Higher Affinity Receptor Binding Dot Plots for Human Receptors 0 5 10 15 20 25 30 35 40 45 50 Receptor Affinity (K i ( nM )) D 1 a 2b a 2c SERT D3 NET 5 - HT 2c a 1a M 1 a 1b H 1 5 - HT 2a 5 - HT 2b Cyclobenzaprine Norcyclobenzaprine
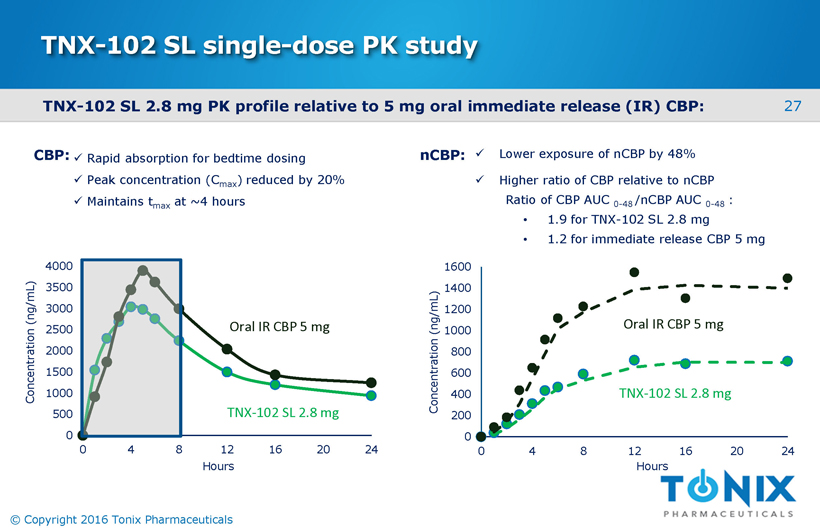
27 © Copyright 2016 Tonix Pharmaceuticals TNX - 102 SL 2.8 mg PK p rofile relative to 5 mg oral immediate release (IR) CBP: TNX - 102 SL single - dose PK study 0 500 1000 1500 2000 2500 3000 3500 4000 0 4 8 12 16 20 24 Concentration (ng/mL) TNX - 102 SL 2.8 mg Oral IR CBP 5 mg x Lower exposure of nCBP by 48% x Higher ratio of CBP relative to nCBP Ratio of CBP AUC 0 - 48 /nCBP AUC 0 - 48 : • 1.9 for TNX - 102 SL 2.8 mg • 1.2 for immediate release CBP 5 mg 0 200 400 600 800 1000 1200 1400 1600 0 4 8 12 16 20 24 Concentration (ng/mL) Oral IR CBP 5 mg TNX - 102 SL 2.8 mg Hours Hours nCBP: x Rapid absorption for bedtime dosing x Peak concentration (C max ) reduced by 20% x Maintains t max at ~4 hours CBP:
28 © Copyright 2016 Tonix Pharmaceuticals TNX - 102 SL: Pharmacokinetic profile after sublingual route of administration • Very rapid absorption after dosing (measurable in plasma within 3 minutes of administration) ‒ Reaching t max at ~4 hours after dosing ‒ Approximately 50% of exposure to cyclobenzaprine occurs during first 8 hours • Avoids first - pass hepatic metabolism to long - lived major metabolite , norcyclobenzaprine ‒ Large reduction in exposure to norcyclobenzaprine ( ↓ 48% AUC 0 - 48 ) ‒ Decreased potential for adverse events
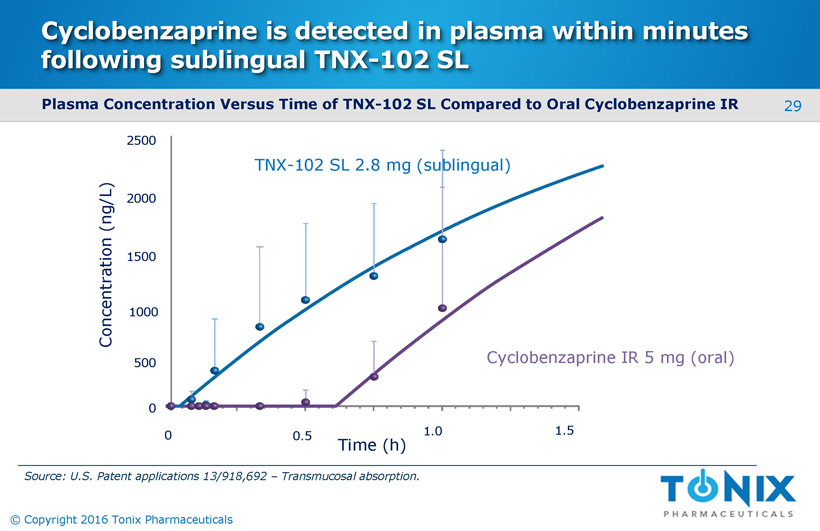
29 © Copyright 2016 Tonix Pharmaceuticals Cyclobenzaprine is detected in plasma within minutes following sublingual TNX - 102 SL Plasma Concentration Versus Time of TNX - 102 SL Compared to Oral Cyclobenzaprine IR 0 0.5 1.0 1.5 Concentration (ng/L) 2500 1500 1000 500 2000 0 TNX - 102 SL 2.8 mg (sublingual) Cyclobenzaprine IR 5 mg (oral) Time (h) Source: U.S. Patent applications 13/918,692 – Transmucosal absorption.

30 © Copyright 2016 Tonix Pharmaceuticals Management team Seth Lederman, MD President & CEO Jessica Edgar Morris EVP, Operations Bruce Daugherty, PhD, MBA Chief Scientific Officer Ronald Notvest, PhD EVP, Commercial Planning & Development Gregory Sullivan, MD Chief Medical Officer Bradley Saenger, CPA Chief Financial Officer
31 © Copyright 2016 Tonix Pharmaceuticals Board of directors Seth Lederman, MD Chairman Ernest Mario, PhD ALZA, Glaxo, Reliant Pharma John Rhodes NYSERDA, NRDC, Booz Allen Hamilton Samuel Saks, MD Jazz Pharma, ALZA, Johnson & Johnson Charles Mather BTIG, Janney, Jefferies, Cowen, Smith Barney Stuart Davidson Labrador Ventures, Alkermes , Combion Patrick Grace Apollo Philanthropy, WR Grace, Chemed Donald Landry, MD, PhD Chair of Medicine, Columbia University
32 © Copyright 2016 Tonix Pharmaceuticals Milestones – recent and upcoming TNX - 102 SL – Posttraumatic Stress Disorder □ December 2015 Entered into Collaborative Research and Development Agreement (CRADA) with the United States Army Medical Materiel Development Activity (USAMMDA) □ May 2016 Report results from AtEase study □ August 2016 End of Phase 2 meeting with FDA - Proposed Phase 3 and NDA plan accepted - Breakthrough Therapy Designation Request can be submitted for review □ Q1 2017 Target commencement of Phase 3 study in military - related PTSD □ 2H 2017 Topline data from interim analysis of Phase 3 study in ~180 military - related PTSD patients x x x
© Copyright 2016 Tonix Pharmaceuticals - Confidential - Do not duplicate or distribute NASDAQ: TNXP 509 Madison Avenue New York, NY 10022 (212) 980 - 9155 www.tonixpharma.com