Tonix Pharmaceuticals Holding Corp. 8-K
Exhibit 99.02
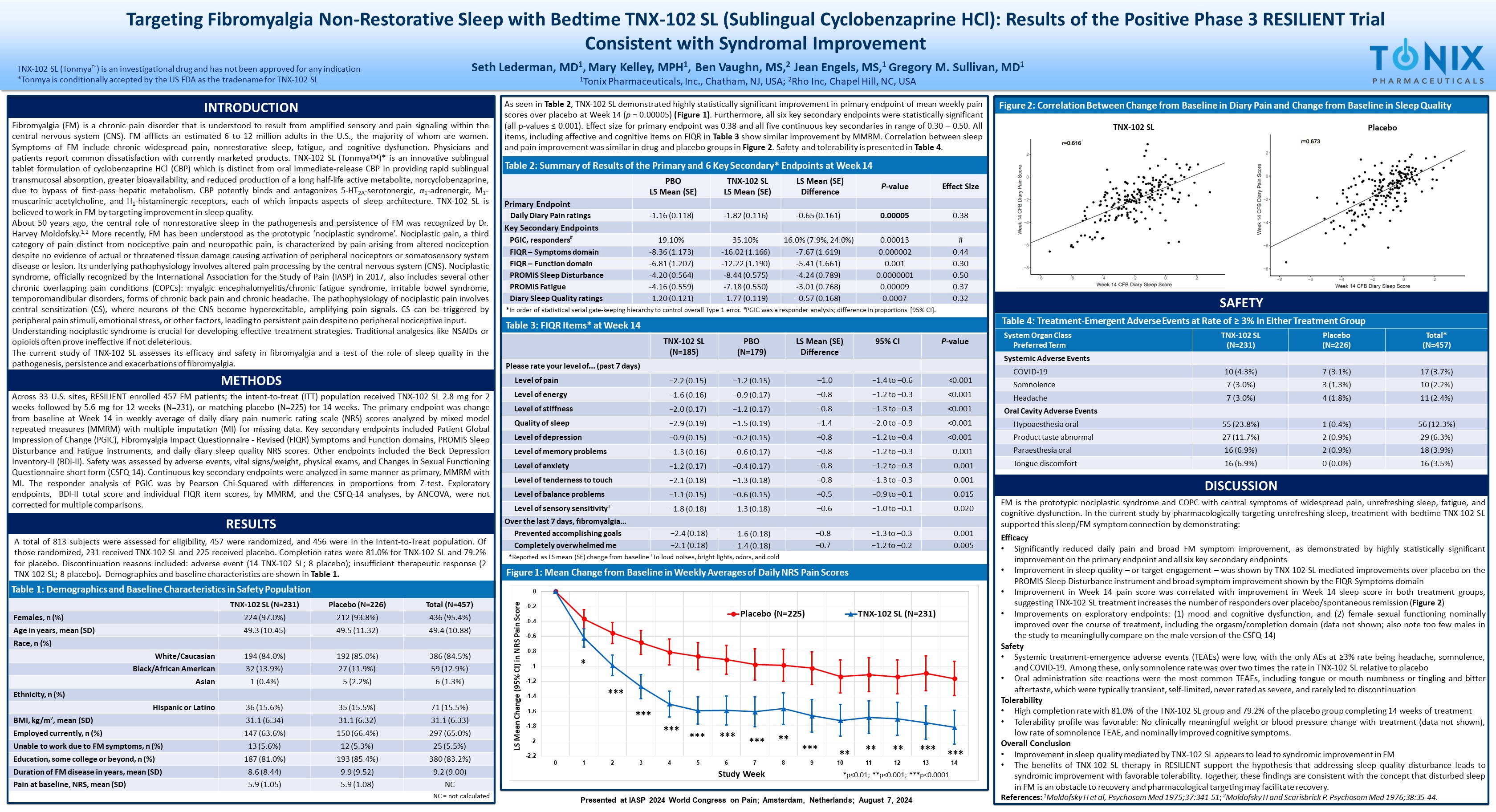
Targeting Fibromyalgia Non - Restorative Sleep with Bedtime TNX - 102 SL (Sublingual Cyclobenzaprine HCl): Results of the Positive P hase 3 RESILIENT Trial Consistent with Syndromal Improvement Seth Lederman, MD 1 , Mary Kelley, MPH 1 , Ben Vaughn, MS, 2 Jean Engels, MS, 1 Gregory M. Sullivan, MD 1 1 Tonix Pharmaceuticals, Inc., Chatham, NJ, USA; 2 Rho Inc, Chapel Hill, NC, USA TNX - 102 SL (Tonmya ) is an investigational drug and has not been approved for any indication *Tonmya is conditionally accepted by the US FDA as the tradename for TNX - 102 SL INTRODUCTION Fibromyalgia (FM) is a chronic pain disorder that is understood to result from amplified sensory and pain signaling within the central nervous system (CNS) . FM afflicts an estimated 6 to 12 million adults in the U . S . , the majority of whom are women . Symptoms of FM include chronic widespread pain, nonrestorative sleep, fatigue, and cognitive dysfunction . Physicians and patients report common dissatisfaction with currently marketed products . TNX - 102 SL ( Tonmya )* is an innovative sublingual tablet formulation of cyclobenzaprine HCl (CBP) which is distinct from oral immediate - release CBP in providing rapid sublingual transmucosal absorption, greater bioavailability, and reduced production of a long half - life active metabolite, norcyclobenzaprine, due to bypass of first - pass hepatic metabolism . CBP potently binds and antagonizes 5 - HT 2 A - serotonergic, α 1 - adrenergic, M 1 - muscarinic acetylcholine, and H 1 - histaminergic receptors, each of which impacts aspects of sleep architecture . TNX - 102 SL is believed to work in FM by targeting improvement in sleep quality . About 50 years ago, t he central role of nonrestorative sleep in the pathogenesis and persistence of FM was recognized by Dr . Harvey Moldofsky . 1 , 2 More recently, FM has been understood as the prototypic ‘ nociplastic syndrome’ . Nociplastic pain, a third category of pain distinct from nociceptive pain and neuropathic pain, is characterized by pain arising from altered nociception despite no evidence of actual or threatened tissue damage causing activation of peripheral nociceptors or somatosensory system disease or lesion . Its underlying pathophysiology involves altered pain processing by the central nervous system (CNS) . Nociplastic syndrome, officially recognized by the International Association for the Study of Pain (IASP) in 2017 , also includes several other chronic overlapping pain conditions (COPCs) : myalgic encephalomyelitis/chronic fatigue syndrome, irritable bowel syndrome, temporomandibular disorders, forms of chronic back pain and chronic headache . The pathophysiology of nociplastic pain involves central sensitization (CS), where neurons of the CNS become hyperexcitable, amplifying pain signals . CS can be triggered by peripheral pain stimuli, emotional stress, or other factors, leading to persistent pain despite no peripheral nociceptive input . Understanding nociplastic syndrome is crucial for developing effective treatment strategies . T raditional analgesics like NSAIDs or opioids often prove ineffective if not deleterious . The current study of TNX - 102 SL assesses its efficacy and safety in fibromyalgia and a test of the role of sleep quality in the pathogenesis, persistence and exacerbations of fibromyalgia . METHODS Across 33 U . S . sites, RESILIENT enrolled 457 FM patients ; the intent - to - treat (ITT) population received TNX - 102 SL 2 . 8 mg for 2 weeks followed by 5 . 6 mg for 12 weeks (N= 231 ), or matching placebo (N= 225 ) for 14 weeks . The primary endpoint was change from baseline at Week 14 in weekly average of daily diary pain numeric rating scale (NRS) scores analyzed by mixed model repeated measures (MMRM) with multiple imputation (MI) for missing data . Key secondary endpoints included Patient Global Impression of Change (PGIC), Fibromyalgia Impact Questionnaire - Revised (FIQR) Symptoms and Function domains, PROMIS Sleep Disturbance and Fatigue instruments, and daily diary sleep quality NRS scores . Other endpoints included the Beck Depression Inventory - II (BDI - II) . Safety was assessed by adverse events, vital signs/weight, physical exams, and Changes in Sexual Functioning Questionnaire short form (CSFQ - 14 ) . Continuous key secondary endpoints were analyzed in same manner as primary, MMRM with MI . The responder analysis of PGIC was by Pearson Chi - Squared with differences in proportions from Z - test . Exploratory endpoints, BDI - II total score and individual FIQR item scores, by MMRM, and the CSFQ - 14 analyses, by ANCOVA, were not corrected for multiple comparisons . RESULTS As seen in Table 2 , TNX - 102 SL demonstrated highly statistically significant improvement in primary endpoint of mean weekly pain scores over placebo at Week 14 ( p = 0 . 00005 ) (Figure 1 ) . Furthermore, all six key secondary endpoints were statistically significant (all p - values ≤ 0 . 001 ) . Effect size for primary endpoint was 0 . 38 and all five continuous key secondaries in range of 0 . 30 – 0 . 50 . All items, including affective and cognitive items on FIQR in Table 3 show similar improvement by MMRM . Correlation between sleep and pain improvement was similar in drug and placebo groups in Figure 2 . Safety and tolerability is presented in Table 4 . Figure 1: Mean Change from Baseline in Weekly Averages of Daily NRS Pain Scores Table 4: Treatment - Emergent Adverse Events at Rate of ≥ 3% in Either Treatment Group Total* (N=457) Placebo (N=226) TNX - 102 SL (N=231) System Organ Class Preferred Term Systemic Adverse Events 17 (3.7%) 7 (3.1%) 10 (4.3%) COVID - 19 10 (2.2%) 3 (1.3%) 7 (3.0%) Somnolence 11 (2.4%) 4 (1.8%) 7 (3.0%) Headache Oral Cavity Adverse Events 56 (12.3%) 1 (0.4%) 55 (23.8%) Hypoaesthesia oral 29 (6.3%) 2 (0.9%) 27 (11.7%) Product taste abnormal 18 (3.9%) 2 (0.9%) 16 (6.9%) Paraesthesia oral 16 (3.5%) 0 (0.0%) 16 (6.9%) Tongue discomfort SAFETY FM is the prototypic nociplastic syndrome and COPC with central symptoms of widespread pain, unrefreshing sleep, fatigue, and cognitive dysfunction . In the current study b y pharmacologically targeting unrefreshing sleep, treatment with bedtime TNX - 102 SL supported this sleep/FM symptom connection by demonstrating : Efficacy • Significantly reduced daily pain and broad FM symptom improvement, as demonstrated by highly statistically significant improvement on the primary endpoint and all six key secondary endpoints • Improvement in sleep quality – or target engagement – was shown by TNX - 102 SL - mediated improvements over placebo on the PROMIS Sleep Disturbance instrument and broad symptom improvement shown by the FIQR Symptoms domain • Improvement in Week 14 pain score was correlated with improvement in Week 14 sleep score in both treatment groups, suggesting TNX - 102 SL treatment increases the number of responders over placebo/spontaneous remission ( Figure 2 ) • Improvements on exploratory endpoints : ( 1 ) mood and cognitive dysfunction, and ( 2 ) female sexual functioning nominally improved over the course of treatment, including the orgasm/completion domain (data not shown ; also note too few males in the study to meaningfully compare on the male version of the CSFQ - 14 ) Safety • Systemic treatment - emergence adverse events (TEAEs) were low, with the only AEs at ≥ 3 % rate being headache, somnolence, and COVID - 19 . Among these, only somnolence rate was over two times the rate in TNX - 102 SL relative to placebo • Oral administration site reactions were the most common TEAEs, including tongue or mouth numbness or tingling and bitter aftertaste, which were typically transient, self - limited, never rated as severe, and rarely led to discontinuation Tolerability • High completion rate with 81 . 0 % of the TNX - 102 SL group and 79 . 2 % of the placebo group completing 14 weeks of treatment • Tolerability profile was favorable : No clinically meaningful weight or blood pressure change with treatment (data not shown), low rate of somnolence TEAE, and nominally improved cognitive symptoms . Overall Conclusion • Improvement in sleep quality mediated by TNX - 102 SL appears to lead to syndromic improvement in FM • The benefits of TNX - 102 SL therapy in RESILIENT support the hypothesis that addressing sleep quality disturbance leads to syndromic improvement with favorable tolerability . Together, these findings are consistent with the concept that disturbed sleep in FM is an obstacle to recovery and pharmacological targeting may facilitate recovery . References : 1 Moldofsky H et al, Psychosom Med 1975 ; 37 : 341 - 51 ; 2 Moldofsky H and Scarisbrick P . Psychosom Med 1976 ; 38 : 35 - 44 . DISCUSSION Table 3: FIQR Items* at Week 14 P - value 95% CI LS Mean (SE) Difference PBO (N=179) TNX - 102 SL (N=185) Please rate your level of... (past 7 days) <0.001 −1.4 to – 0.6 – 1.0 −1.2 (0.15) −2.2 (0.15) Level of pain <0.001 −1.2 to – 0.3 – 0.8 −0.9 (0.17) −1.6 (0.16) Level of energy <0.001 −1.3 to – 0.3 – 0.8 −1.2 (0.17) −2.0 (0.17) Level of stiffness <0.001 −2.0 to – 0.9 – 1.4 −1.5 (0.19) −2.9 (0.19) Quality of sleep <0.001 −1.2 to – 0.4 – 0.8 −0.2 (0.15) −0.9 (0.15) Level of depression 0.001 −1.2 to – 0.3 – 0.8 −0.6 (0.17) −1.3 (0.16) Level of memory problems 0.001 −1.2 to – 0.3 – 0.8 −0.4 (0.17) −1.2 (0.17) Level of anxiety 0.001 −1.3 to – 0.3 – 0.8 −1.3 (0.18) −2.1 (0.18) Level of tenderness to touch 0.015 −0.9 to – 0.1 – 0.5 −0.6 (0.15) −1.1 (0.15) Level of balance problems 0.020 −1.0 to – 0.1 – 0.6 −1.3 (0.18) −1.8 (0.18) Level of sensory sensitivity † Over the last 7 days, fibromyalgia… 0.001 −1.3 to – 0.3 – 0.8 −1.6 (0.18) −2.4 (0.18) Prevented accomplishing goals 0.005 −1.2 to – 0.2 – 0.7 −1.4 (0.18) −2.1 (0.18) Completely overwhelmed me Table 2: Summary of Results of the Primary and 6 Key Secondary* Endpoints at Week 14 Effect Size P - value LS Mean (SE) Difference TNX - 102 SL LS Mean (SE) PBO LS Mean (SE) Primary Endpoint 0.38 0.00005 - 0.65 (0.161) - 1.82 (0.116) - 1.16 (0.118) Daily Diary Pain ratings Key Secondary Endpoints # 0.00013 16.0% (7.9%, 24.0%) 35.10% 19.10% PGIC, responders # 0.44 0.000002 - 7.67 (1.619) - 16.02 (1.166) - 8.36 (1.173) FIQR – Symptoms domain 0.30 0.001 - 5.41 (1.661) - 12.22 (1.190) - 6.81 (1.207) FIQR – Function domain 0.50 0.0000001 - 4.24 (0.789) - 8.44 (0.575) - 4.20 (0.564) PROMIS Sleep Disturbance 0.37 0.00009 - 3.01 (0.768) - 7.18 (0.550) - 4.16 (0.559) PROMIS Fatigue 0.32 0.0007 - 0.57 (0.168) - 1.77 (0.119) - 1.20 (0.121) Diary Sleep Quality ratings -2.2 -2 -1.8 -1.6 -1.4 -1.2 -1 -0.8 -0.6 -0.4 -0.2 0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 LS Mean Change (95% CI) in NRS Pain Score Study Week Placebo (N=225) TNX-102 SL (N=231) * *** *** ** ** ** *** *** *** *** *** *** *** ** A total of 813 subjects were assessed for eligibility, 457 were randomized, and 456 were in the Intent - to - Treat population . Of those randomized, 231 received TNX - 102 SL and 225 received placebo . Completion rates were 81 . 0 % for TNX - 102 SL and 79 . 2 % for placebo . Discontinuation reasons included : adverse event ( 14 TNX - 102 SL ; 8 placebo) ; insufficient therapeutic response ( 2 TNX - 102 SL ; 8 placebo) . Demographics and baseline characteristics are shown in Table 1 . * In order of statistical serial gate - keeping hierarchy to control overall Type 1 error. # PGIC was a responder analysis; difference in proportions [95% CI]. Table 1: Demographics and Baseline Characteristics in Safety Population Total (N=457) Placebo (N=226) TNX - 102 SL (N=231) 436 (95.4%) 212 (93.8%) 224 (97.0%) Females, n (%) 49.4 (10.88) 49.5 (11.32) 49.3 (10.45) Age in years, mean (SD) Race, n (%) 386 (84.5%) 192 (85.0%) 194 (84.0%) White/Caucasian 59 (12.9%) 27 (11.9%) 32 (13.9%) Black/African American 6 (1.3%) 5 (2.2%) 1 (0.4%) Asian Ethnicity, n (%) 71 (15.5%) 35 (15.5%) 36 (15.6%) Hispanic or Latino 31.1 (6.33) 31.1 (6.32) 31.1 (6.34) BMI, kg/m 2 , mean (SD) 297 (65.0%) 150 (66.4%) 147 (63.6%) Employed currently, n (%) 25 (5.5%) 12 (5.3%) 13 (5.6%) Unable to work due to FM symptoms, n (%) 380 (83.2%) 193 (85.4%) 187 (81.0%) Education, some college or beyond, n (%) 9.2 (9.00) 9.9 (9.52) 8.6 (8.44) Duration of FM disease in years, mean (SD) NC 5.9 (1.08) 5.9 (1.05) Pain at baseline, NRS, mean (SD) NC = not calculated *p<0.01; **p<0.001; ***p<0.0001 Figure 2: Correlation Between Change from Baseline in Diary Pain and Change from Baseline in Sleep Quality TNX - 102 SL Placebo Presented at IASP 2024 World Congress on Pain; Amsterdam, Netherlands; August 7, 2024 *Reported as LS mean (SE) change from baseline † To loud noises, bright lights, odors, and cold